Poster
Contents
| INABIS '98 Home Page | Your Poster Session | Related Symposia & Posters | Scientific Program | Exhibitors' Foyer | Personal Itinerary | New Search |
Clinical course
 Click to enlarge
Fig. 3: Clinical course.
Click to enlarge
Fig. 3: Clinical course.
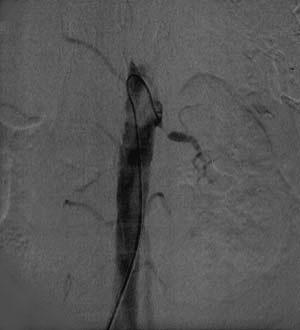
As shown in Fig 3, we chose hydroxyurea to decrease her blood count at first. As BUN was increased we changed it to SPAC (cytarabine ocfosfate). But increasing of BUN continued, and she needed admission. After admission we stopped the administration of any anticancer agents, because we thought the possibility of drug induced acute renal failure. But her renal dysfunction did not improved. Finally BUN and Cr was up to 85 mg/dl and 7.2 mg/dl respectively. therefore hemodyalisis (HD) was performed. We concluded that the drugs did not cause the renal failure. She had an examination of angiography, which showed bilateral renal artery occlusion. (Fig 4)
 Click to enlarge
Fig. 4: Renal artery angiography.
Click to enlarge
Fig. 4: Renal artery angiography.
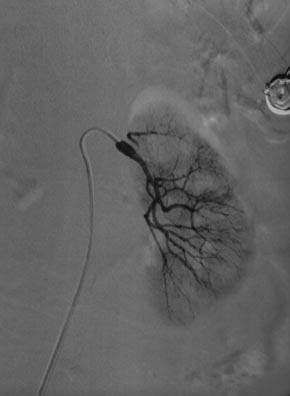
She successfully underwent percutaneous transluminal angioplasty (PTA), and the left renal artery was recanalised. (Fig 5)
 Click to enlarge
Fig. 5: Post angioplasty.
Click to enlarge
Fig. 5: Post angioplasty.
From this point BUN and Cr improved rapidly. She needed no more HD treatment (Fig 3). She was treated by antithrombotic agents (ticropidine 200 mg/day and aspirin 81 mg/day) and discharged. Six months later she had no recurrence of renal failure.
| <=Case | CLINICAL COURSE | Discussion & Conclusion=> |
| Discussion Board | Next Page | Your Poster Session |