Neuroscience Poster Session
| INABIS '98 Home Page | Your Session | Symposia & Poster Sessions | Plenary Sessions | Exhibitors' Foyer | Personal Itinerary | New Search |
Introduction
The cerebellum has complex functions concerned with sensorimotor integration and therefore plays important roles in movement control by refining the motor command with temporal and spatial parameters (1-3). All the inputs and outputs of the cerebellum are conducted via bilaterally paired cerebellar peduncles. Despite the homogeneous cortical structure of the cerebellum, specific motor functions can be ascribed to its functional compartments.
In previous studies, we suggested that lesions in the cortico-cerebello-thalamo-cortical pathway was the primary suspect being responsible for action tremor (AT) and impaired control of visually-guided tracking movements in patients with multiple sclerosis (MS)(4); and AT was weighted predominantly at the distal joint of the arm (5). A major difficulty in interpreting our previous results in a group of patients was that the variable nature of MS in the size, number and localisation of demyelinating lesions not only produced great variations between the patients we studied, but made almost impossible to correlate any specific motor deficits with those multiple and dispersed lesions. Focal lesions, however, provide valuable pathological models for correlating specific impairments in sensorimotor behaviour with certain functional sub-units in the cerebellar connections (6-8).
In the present report, we, therefore, investigated specific impairments in the control of visually guided ramp tracking movements and of pre-programmed pointing movements in one selected patient who had focal MS lesions in the cerebellum and brainstem clearly defined by magnetic resonance imaging (MRI).
Materials and Methods
The patient and normal controls:
A male patient, aged 46, right-handed, had a diagnosis of laboratory-supported definite MS. His major complaints were shaking in the upper limbs, inability to roll a cigarette, and unsteadiness when standing and walking. Clinically, AT, dysdiadochokinesis in the upper limbs, disequilibrium and weakness while standing and walking, and reduced sensation from the knees down were revealed. Subtle left internuclear ophthalmoplegia, but no severe nystagmus or diplopia which would interfere with the perception of the visual cues were found. Five healthy subjects without neurological deficits were also tested as normal controls. Ethical approval was obtained for these studies.
MRI scans:
MRI scans were carried out at the John Radcliffe Hospital, Oxford. Focal lesions were revealed by T2-weighted MRI images (TR 4055.0ms, TE 90.0/2, 10mm slices). Precise location of lesions was identified by comparing MRI pictures with a colour anatomic atlas (9).
Visually-guided motor tasks:
- "On-line" wrist and arm ramp tracking tasks: A 12x12 pixel hollow square target moved either horizontally (for wrist tracking and reaction time measurement) or circularly (for arm tracking) at a constant speed on a computer screen. The patient moved a low-resistance joystick to control a continuously displayed cursor either a) by wrist flexion and extension with the forearm supported in an plastic splint or b) by arm moving around at the shoulder joint while keeping the elbow straight.(4 5) The voltage signals generated by the joystick in each tracking task were recorded. The severity of AT was quantified by calculating the standard deviation of the movement velocity (SD-MV). Accuracy of tracking movement was measured as the absolute percentage error in the movement velocity (EV) relative to the target velocity. For perfect, smooth tracking the SD-MV and EV would be zero and 0%, respectively. The frequency composition of the tracking records was also computed using the fast-Fourier-transform. Visually-cued simple reaction times (SRT) were also measured using the wrist tracking equipment. AT was differentiated as distal or proximal tremor using the ratio of SD-MV in the wrist tracking relative to that in arm tracking.
- "Off-line" arm pointing task: The subject was instructed to move the right arm in a single movement from a constant starting position to reach one of three visual targets presented 20cm away on a digitising board. View of the moving arm was blocked, and instead the arm position was indicated using a visual cursor displayed only at the completion of the movement (10). Pointing movements were digitally recorded while the ratio between movement amplitude and the visual feedback was modified with a single-step gain change from 1 to 1.5 times. The target/movement amplitude ratio (TM ratio) was calculated to quantify each movement of the subject's pointing. Spatial variability (SV) in final position of each movement along the movement direction was calculated as the standard deviation of the TM ratio, and expressed as a percentage of the mean TM ratio. For perfect pointing without a gain change, the TM ratio and SV would be 100% and 0%. Adaptation to the gain change was measured as the percentage change in TM ratio between movements before and after the gain change in the visual feedback. For perfect adaptation, the change in TM ratio would equal to the change in visual gain (i.e. 100%). Finally, random visual "noise" was added to the cursor position in some sessions by shifting randomly, on a trial-to-trial basis, the position of the cursor. The level of noise was varied from �10%, �30%, �50%, �75% and �100% of the movement amplitude, and its effect on gain adaptation accessed.
Results
Anatomic location of lesions: Multiple focal lesions of hyperintense signal and a few millimetres in diameter were seen in the white matter of the right cerebellar hemisphere and bilaterally in the inferior/middle cerebellar peduncles (Figure, left half), and the right cerebral peduncle (Figure, right half). The lesions in the right cerebellum were located latero-ventrally around the dentate nucleus, and thus would primarily affect the efferent fibres from the ipsilateral cerebellar cortex. In addition, afferent fibres from the brainstem to the cerebellum could have been affected. The lesions in the bilateral inferior/middle peduncles would have disrupted connections between the cerebellum and neighbouring brainstem structures, including the lateral and inferior vestibular nuclei, reticular formations and the inferior olive. The focal lesion in the right cerebral peduncle would have damaged part of the cerebrospinal tract.
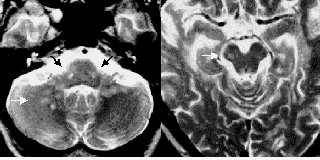 Figure: T2-weighted MRI scan revealed that multiple focal lesions of a few millimetres in diameter with high signal in the white matter ventrally around the right dentate nuclei (white arrow, left half), the centres of bilateral inferior cerebellar peduncles (black arrows) and right cerebral peduncle in which lateral corticospinal tract fibres were mainly involved (white arrow, right half).
Figure: T2-weighted MRI scan revealed that multiple focal lesions of a few millimetres in diameter with high signal in the white matter ventrally around the right dentate nuclei (white arrow, left half), the centres of bilateral inferior cerebellar peduncles (black arrows) and right cerebral peduncle in which lateral corticospinal tract fibres were mainly involved (white arrow, right half).
Impairments in control of visually guided arm movements: Results of arm tracking and pointing movements from the patient in comparison with normal controls are listed in the table, in which values beyond the 95% confidence range of that in controls are defined as abnormal.
- "On-line" tracking tasks. The patient had AT in both arms reflected by increased SD-MV. There was a pronounced peak at 4Hz in the frequency spectra. The wrist/arm AT ratios were higher than that in normal controls, which suggested that his tremors were predominantly distal in both arms. EV was elevated during right wrist tracking and left arm tracking. Visually cued reaction time was prolonged in both arms.
- "Off-line" pointing tasks. The patient's pointing movements were dysmetric as the SV during pointing to a visual target was increased with respect to controls. However, his average movement amplitude over the baseline trials was not significantly different from that of the normal controls. The level of adaptation of his movement amplitude to a gain change was also within the normal range. The amount of random visual feedback noise that could be tolerated without disturbing his adaptation was considerably higher, as he showed no significant reduction in adaptation with up to �75% random noise, while controls showed a significant reduction in adaptation with only �30% noise.
Table. Motor impairments assessed by visually guided tasks ___________________________________________________________ MS patient Normal controls (mean � SD) ___________________________________________________________ 1. Tracking tasks (n=10) SD-MV (deg/s) Wrist L 184.3* 65.8 � 13.8 R 156.9* Arm L 41.9* 20.7 � 3.2 R 37.4* Wrist/arm AT ratio L 4.4* 3.2 � 0.5 R 4.2* EV (%) Wrist L 2.0* 5.6 � 1.5 R 12.8* Arm L 36.0 12.4 � 12.5 R 0.1 SRT (ms) L 423.1* 264.6 � 23.3 R 403.3* 2. Pointing tasks (n=11) SV (%) R 16.0%* 10.3% � 2.1% Adaptation (%) R 68% 55% � 36.7% Noise threshold (%) R 75% 30% ___________________________________________________________ * Values in the patient are beyond the 95% confidence range (mean � 1.96 SD) in controls.
Discussion and Conclusion
In the present report, we investigated specific impairments in visuomotor behaviour of the arm in "on-line" control of visually guided tracking movements and in the "of-line" control of pre-programmed pointing movements in a patient who had focal MS lesions in the cerebellum and brainstem defined by MRI images. The patient had predominantly distal action tremor in both arms with increased tracking errors and prolonged reaction times. Despite being dysmetric with increased spatial variability during pointing movements, the patient was able to adapt his movements amplitude to a gain change in the visual feedback even in the presence of significant visual "noise".
The bilateral arm AT and disturbances in equilibrium and walking in this patient were very likely caused by the symmetrical lesions in the inferior/middle cerebellar peduncles. These lesions would have damaged the fibres connecting the cerebellum and neighbouring brainstem structures including the lateral and inferior vestibular nuclei, reticular formation and inferior olive. These lesions could also be responsible for his detected internuclear ophthalmoplegia in the left. However, he had no palatal tremor despite the obvious axial involvement in his clinical symptoms. The somatotopy within the cerebellar-brainstem connections proposed by Brown and colleagues8 may be an explanation, as the focal lesions appear to have spared the connections to medial cerebellar areas contributing to oculomotor and palatal control.
Lesions in the cortico-cerebello-thalamo-cortical pathway are the primary suspects for causing distal arm tremor in patients with MS (4,5). MS lesions are believed to primarily involve the white matter, and the lesions in this patient may therefore block the afferents and efferents of the cerebellar nuclei, if not damaging them directly. The patient's on-line closed-loop control of tracking movements may have been further impaired by increased delays in the feedback loop caused by possible conduction blockage. Thus, lesions in this part were mainly responsible for the impaired control of movement timing reflected by the delay in visually cued reaction time and decrease in accuracy of tracking velocity. His tracking behaviour was further disturbed by the effect of his AT on the cursor, adding dramatically to the error between target and cursor. Complimentary to previous studies on patients with cerebellar damages due to brain trauma (6) or stroke (7), we propose that in addition to damage in the superior cerebellar peduncles which contain ascending outflow to the motor cortex, the impaired on-line control of visually guided tracking movement can also occur as a consequence of damage in inferior and middle cerebellar peduncles which contain spinal afferents to the cerebellum and the brain stem-cerebellum connections.
The pointing movements of the patient performed "open-loop" with respect to visual feedback were dysmetric with increased spatial variability in pointing to visual targets. However, the average of his movement amplitudes over a number of trials was not significantly different from that of the normal controls, suggesting that he was able to scale his basic motor commands for pointing to the target; in other words, he was able to program his movements even though he had difficult to execute them accurately. He was able to efficiently adapt his movements when the gain of the "off-line" visual feedback of his movement was modified. Based on the results from our patient and another patient studied by Martin and colleagues (7) on a dart-throwing task, it appears that partial damage in the inferior and middle cerebellar peduncles does not significantly affect adaptation to changes in the visual feedback, nor do lesions to the ipsilateral cerebellar nuclei. Interestingly, our patient was able to adapt with much greater random visual noise superimposed on the visual feedback of his movement position (75%, comparing with 30% in the controls). This may be because his arm movements are normally very variable due to AT and dysmetria. Hence the addition of extra visual noise in the experiment may not be as disturbing as it is for the more consistent controls. Together these indicate that his off-line control for pointing movements was almost intact, i.e. he was able to select meaningful visual information from previous movements even in the presence of extra random noise and update his motor commend appropriately.
Finally, we suspect that the focal lesion in the right cerebral peduncle mainly involving the cerebrospinal tract may be the reason that motor impairments are noticeably worse in the left than right side.
Conclusive remarks: We have used two visually guided movement tasks, one dependent on on-line, and the other on off-line visual feedback to contrast the motor performance of a MS patient with focal cerebellar lesions to normal controls. The patient had severe difficulties in the on-line control of his movements, but near-normal control of adaptation of his off-line controlled movements. These results compliment investigations on the role of the cerebellum in motor control and learning.
References
1. Stein JF. Role of the cerebellum in the visual guidance of movement. Nature 1986;232:217-21.
2. Diener H-C, Dichgans J. Pathophysiology of cerebellar ataxia. Mov Disord 1992;2:95-109.
3. Horne MK, Butler EG. The role of the cerebello-thalamo-cortical pathway in skilled movement. Prog in Neurobiol 1995; 46:199-213.
4. Liu X, Miall RC, Aziz TZ, et al. Analysis of action tremor and impaired control of movement velocity in multiple sclerosis during visually-guided wrist tracking tasks. Mov Disord 1997;12:992-9.
5. Liu X, Miall RC, Aziz TZ, et al. Distal versus proximal arm tremor in multiple sclerosis assessed by visually guided tracking tasks. J Neurol Neurosurg Psychiatry in press.
6. Haggard P, Miall RC, Wade D, et al. Damage to cerebellocortical pathways after closed head injury: A behavioral and magnetic resonance imaging study. J Neurol Neurosurg Psychiatry 1995; 58:433-8.
7. Martin TA, Keating JG, Goodkin HP, et al. Throwing while looking through prisms. I. Focal olivocerebellar lesions impair adaptation. Brain 1996;119:1183-98.
8. Brown P, Rothwell JC, Stevens JM, et al. Cerebellar axial postural tremor. Mov Disord 1997;12: 977-84.
9. England MA, Wakely J. A colour atlas of the brain and spinal cord. Wolfe Publishing Ltd, London, 1991; pp170, 235.
10. Wolpert DM, Ghahramani Z, Jordan MI. Are arm trajectories planned in kinematic or dynamic coordinates? An adaptation study. Exp Brain Res 1995;103:460-70.
| Discussion Board | Previous Page | Your Poster Session |