|
|
Oral & Maxillofacial Service Hospital Universitario "Del Río Hortega" Valladolid. SPAIN |
|
| INABIS '98 Home Page | Your Poster Session | Related Symposia & Posters | Plenary Sessions | Exhibitors' Foyer | Personal Itinerary | New Search |
|
|
Oral & Maxillofacial Service Hospital Universitario "Del Río Hortega" Valladolid. SPAIN |
|
TWO CASES OF TEMPOROMANDIBULAR JOINT ANKYLOSIS TREATMENT BY MEANS OF OSTEOARTRECTOMY AND TEMPORALIS MUSCLE INTERPOSITION FLAP.
Garcia Cantera, JM
, MD, PhD; Perez Gonzalez, E*, MD, Phd; Blanco Rueda, JA, MD, PhD; Izquierdo Millan, M, MD; Garcia Reija, F, MD; Verrier Hernández, A, MD, PhD.Oral & Maxillofacial Surgery Service.
(*) Radiology Service.
Hospital Universitario Rio Hortega.
Valladolid. SPAIN
Contact person:
J.M.García Cantera . e-mail: mcantera@lander.es
Different pathologies can originate mandibular ankylosis that affect the temporomandibular joint (TMJ) as to the surrounding structures. The most commonly associated causes are traumatic (31-98%), local or distant infections (10-49%) and the systemic illnesses (10%), as ankylosing espondylitis, rheumatoid arthritis, lupus erythematous or psoriasis.
They have been described a great variety of surgical techniques for the treatment of the temporomandibular (TMJ) ankylosis, including articular total TMJ replacement prosthesis, as well as multiple homologous interference materials, heterologous and synthetic used to avoid the reankylosis of the dried up bony fragments .
Presented communication describes two surgically treated cases by means of:
1. Aggressive resection of the ankylotic segment.
2. Associated coronoidectomy if is necessary.
3. Interference flap temporalis muscle.
4. Early mobilization and physiotherapy.
Case report 1.
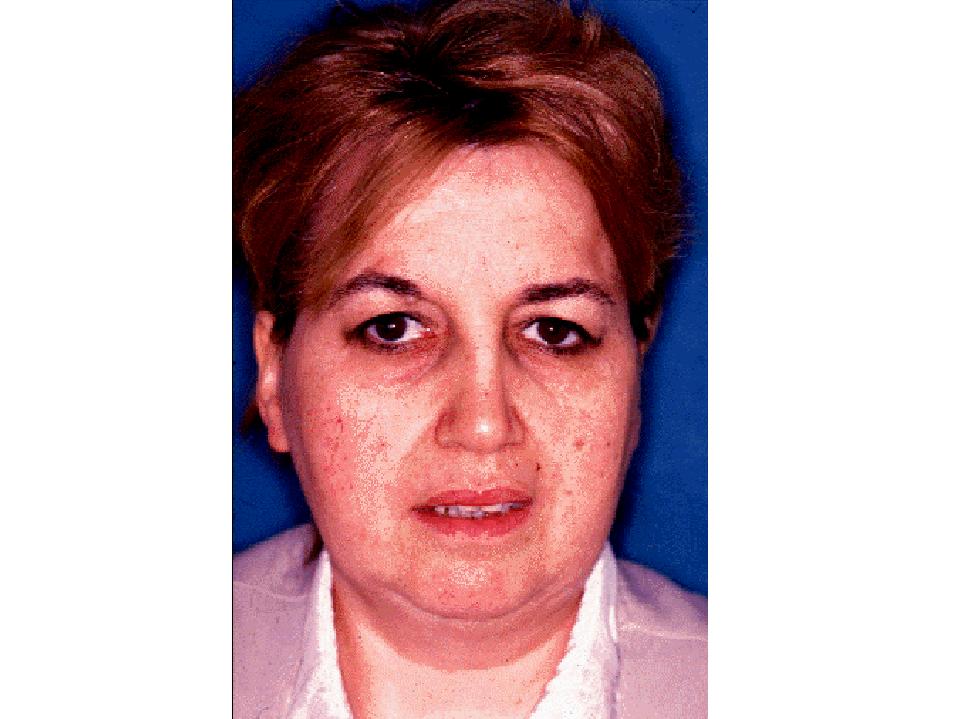
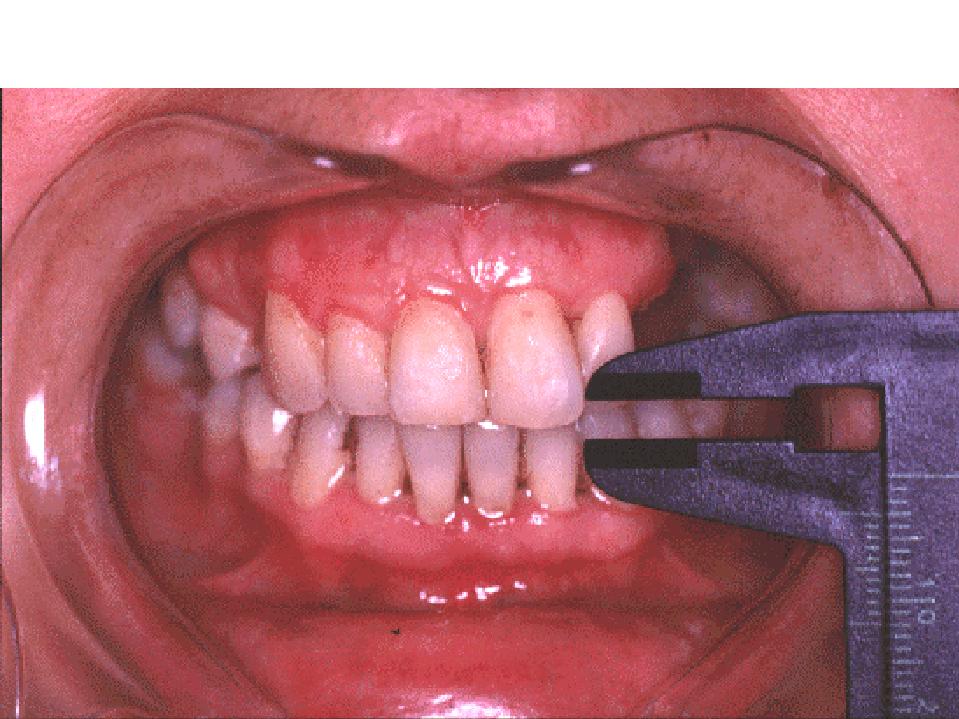
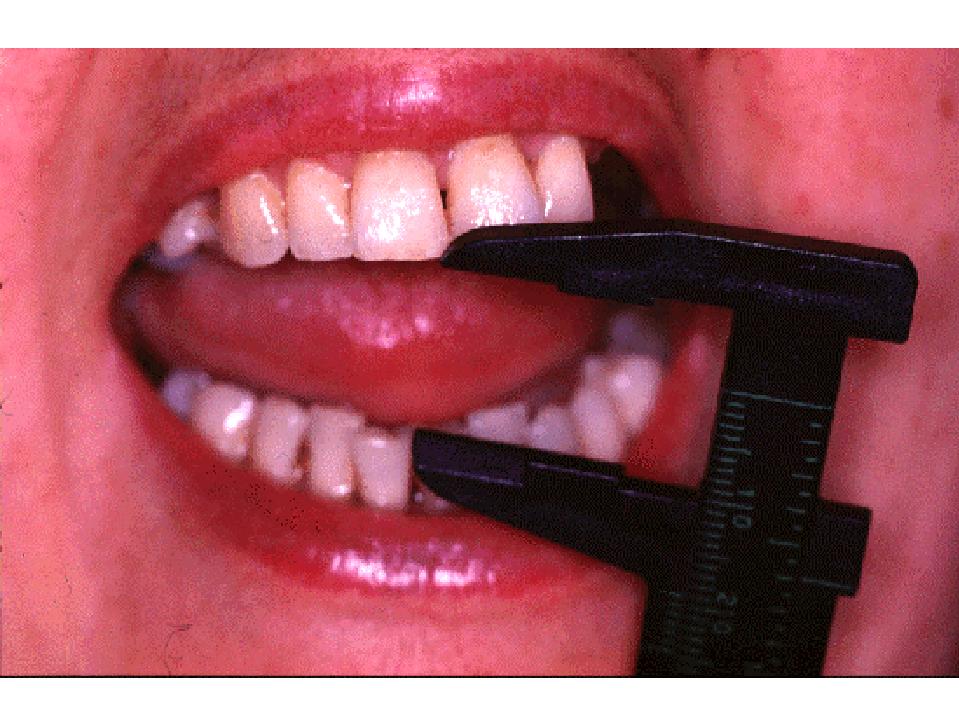
52 year-old woman that presented both ankylosing espondylitis TMJ affectation several years old. Pre-treatment oral opening of 2–3 mm. Difficulty with speech, mastication, oral hygiene and chonic local pain. Post-treatment oral opening: 19 mm. Good functional improvement.
Case report 2.
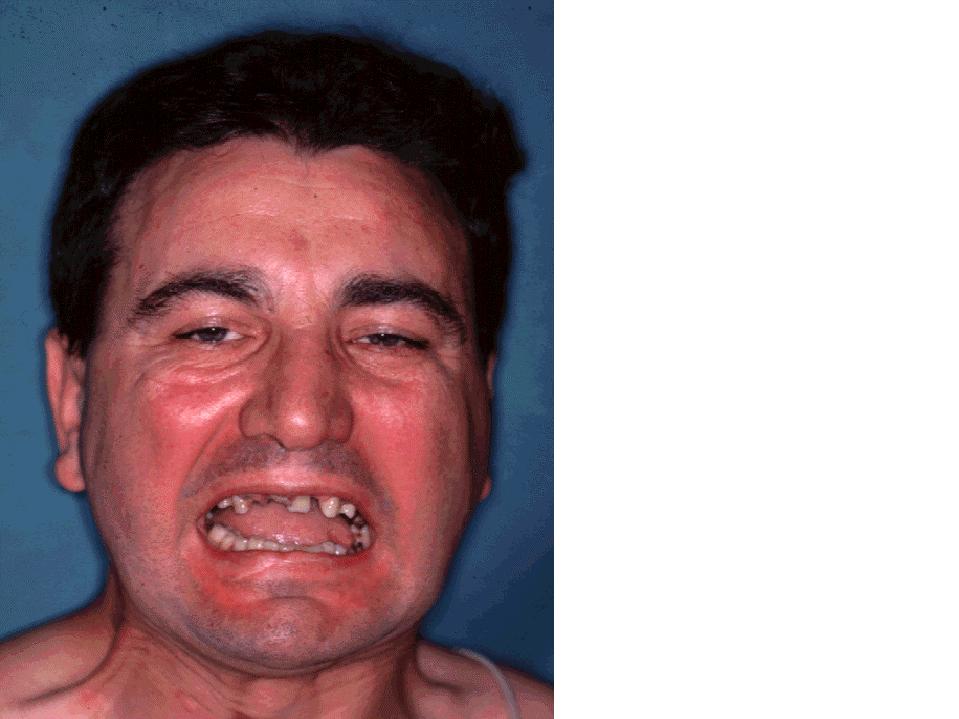
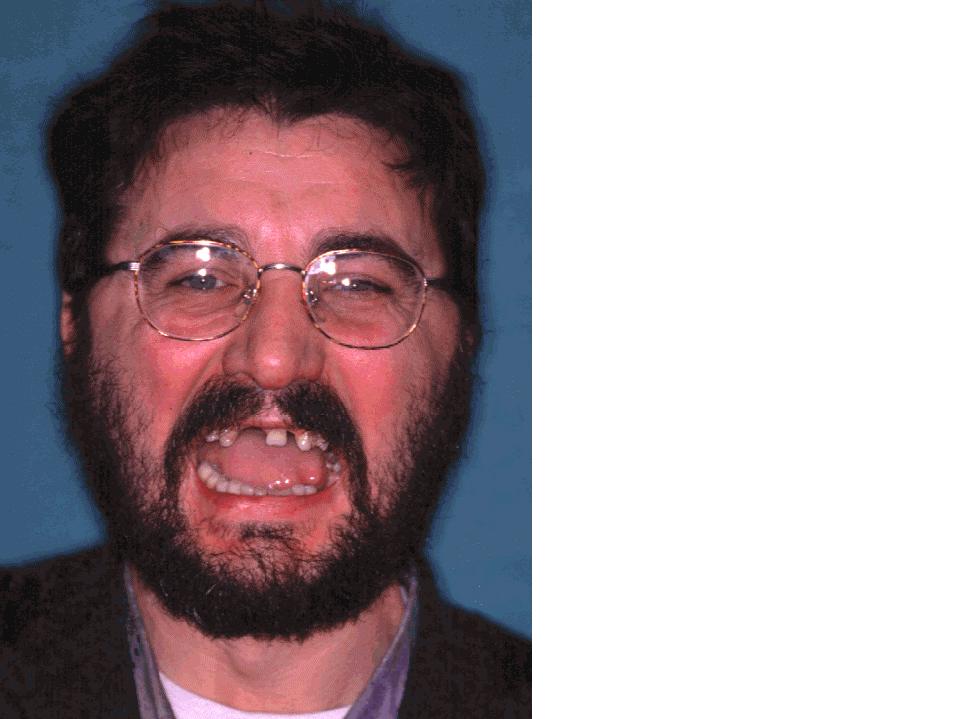
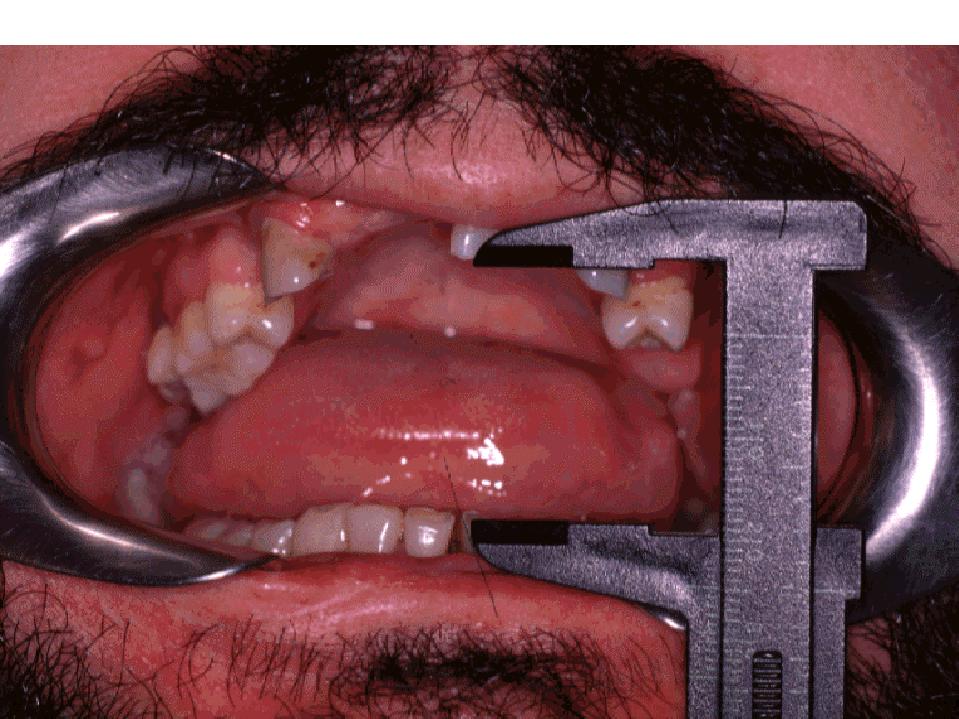
30 year-old male with postraumatic bilateral mandibular ankylosis (old bilateral intracapsular fractures). Oral opening of 12 mm, without condilar translation movement. After surgical treatment and later rehabilitation, the oral opening were 26 mm.
Different pathologies can originate mandibular ankylosis that affect the temporomandibular articulation as to the surrounding structures. The most commonly associated causes are traumatic (31-98%), local or distant infections (10-49%) and the systemic illnesses (10%), as ankylosing espondylitis, rheumatoid arthritis, lupus erythematous or psoriasis.
They have been described a great variety of surgical techniques for the treatment of the temporomandibular (TMJ) ankylosis, including articular total TMJ replacement prosthesis, as well as multiple homologous interference materials, heterologous and synthetic used to avoid the reankylosis of the dried up bony fragments .
We describes two surgically treated cases by means of:
1. Aggressive resection of the ankylotic segment.
2. Associated coronoidectomy if is necessary.
3. Interference flap temporalis muscle.
4. Early mobilization and physiotherapy.
|
|
|
|
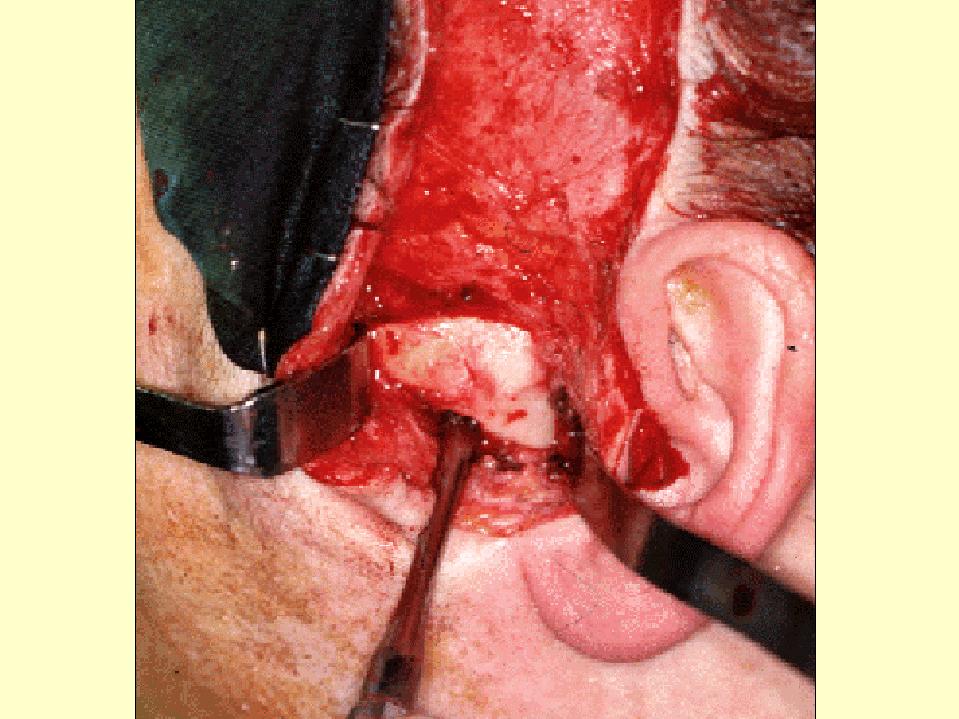
Al Kayat - Bramley type TMJ approache |
Pseudoarticular space |
|
|
|
|
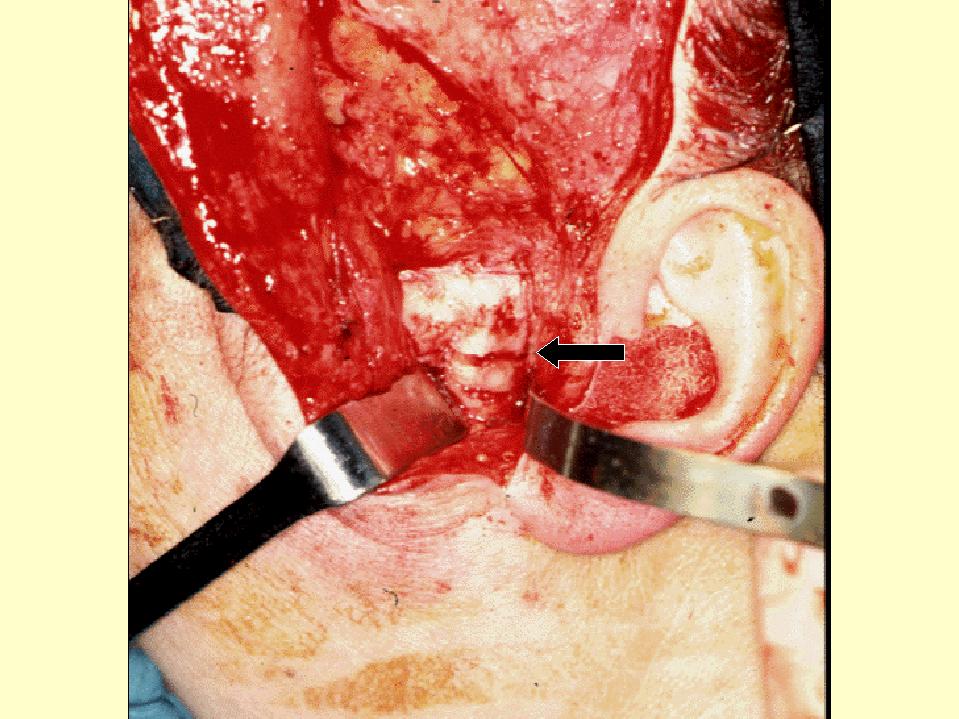
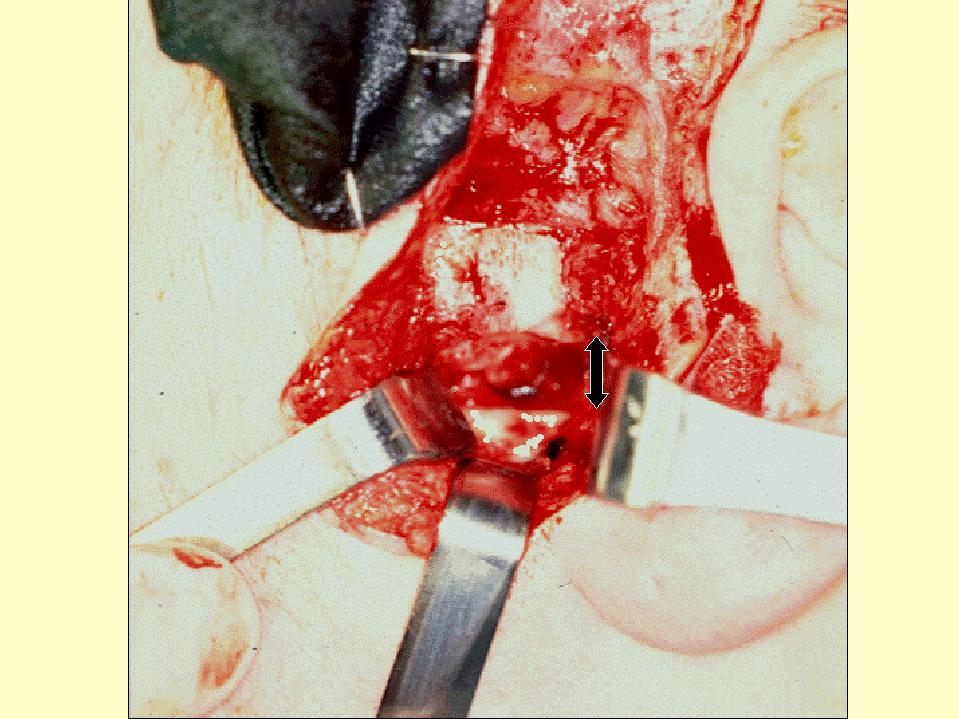
Aggressive resection of the ankylotic segment |
Interposition temporalis muscle flap. |
Results and discussion
Case report 1
|
|
|
52 year-old woman that presented both ankylosing espondylitis TMJ affectation several years old. Pre-treatment interincisal-measurement oral opening of 3 mm. Difficulty with to pronounce, mastication, oral hygiene and chronic local pain. She can´t to chew and has liquid nutrition.
|
|
|
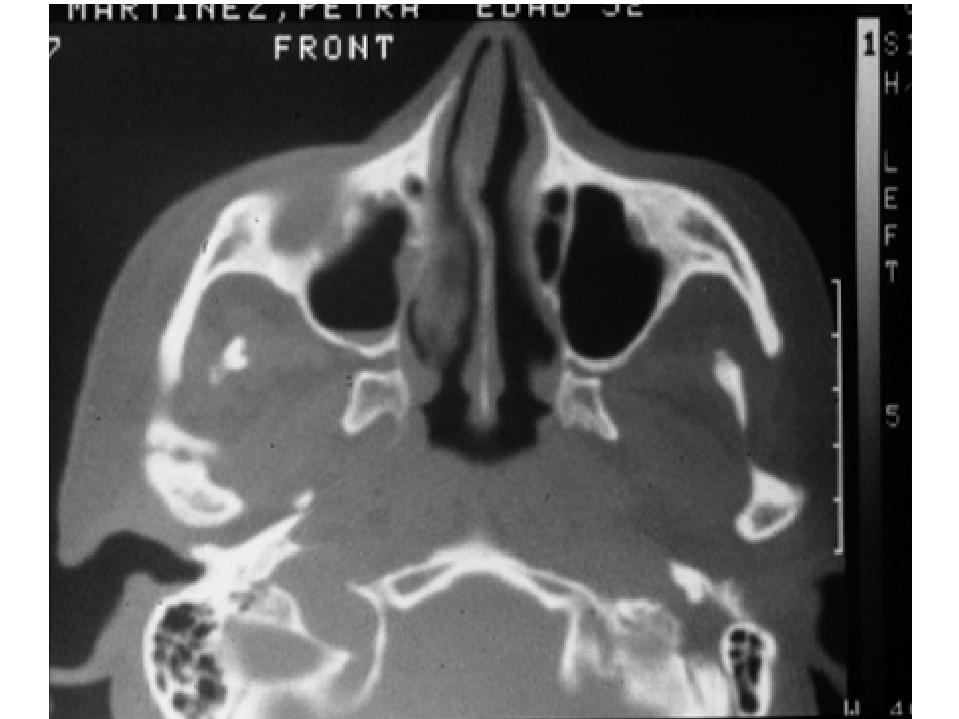
The CT-scan reveals bilateral ankilosys with great reduction of the articular space, presence of intraarticular bony bridges, discal tissue rests that originates a pseudoarticular space, and hypertrophy and deformity to the condilar bone. No overgrowth evidence of coronoid mandibular process
She has fiberoptic intubation, bilateral type Al Kayat - Bramley TMJ approache, 1 cm osteoartrectomy and temporalis muscle flap interposition between the bony segments
|
|
|
|
|
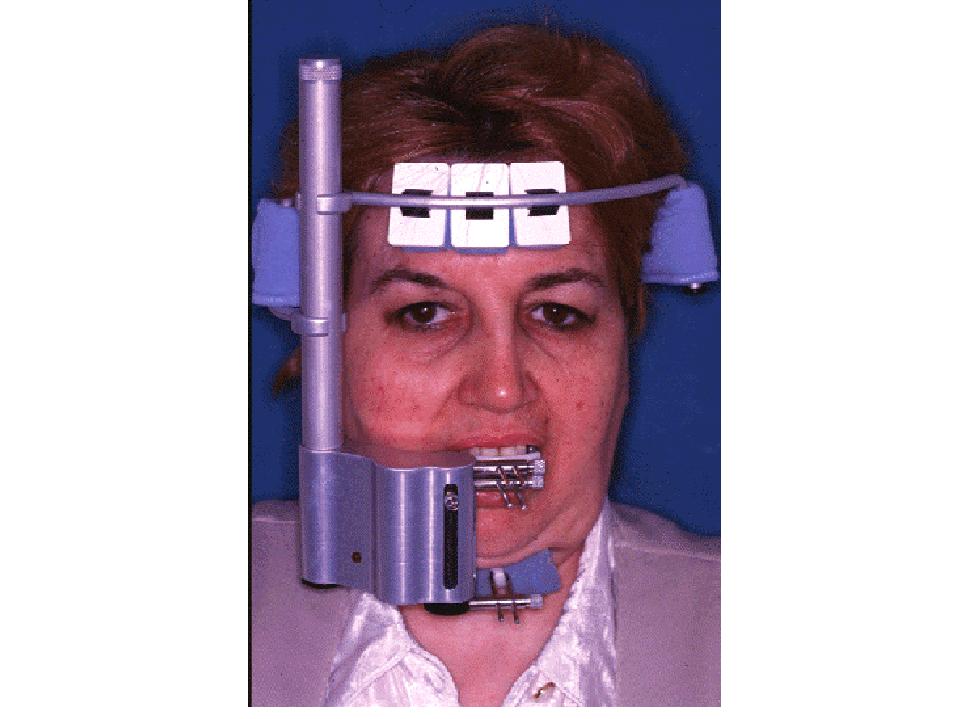
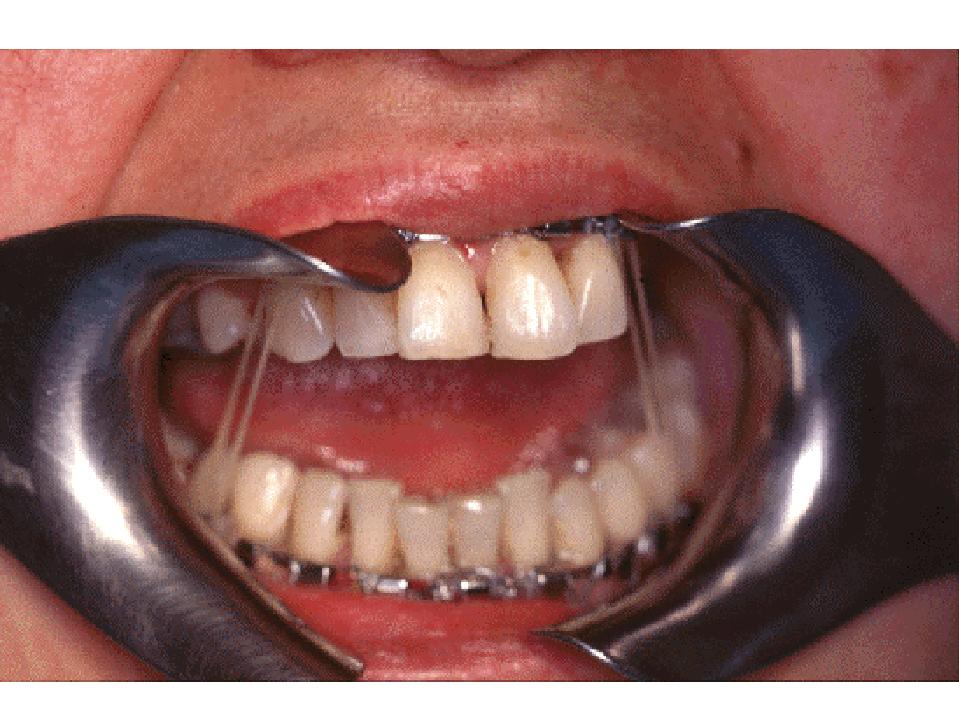
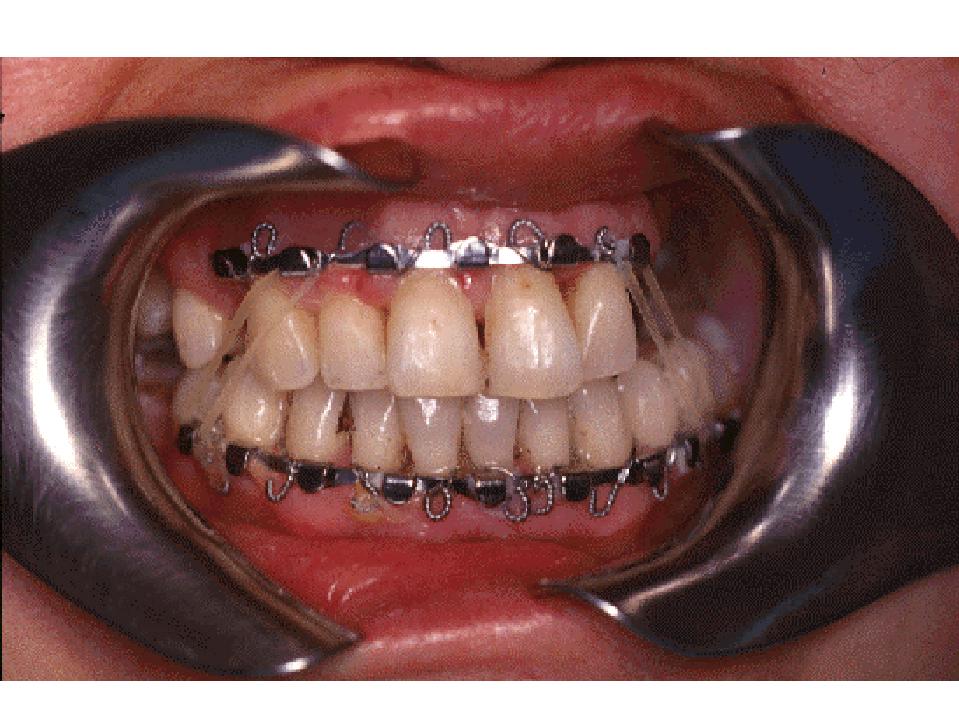
She is carried out precocious mobilization with daily passive exercises (Movilimb J1 TMJ CMP) and active opening and laterotrusive exercices, guiding the occlusion with class III orthodonthic rubbers in the immediate postoperative phase, to reduce the subsequent open bite due to the height reduction of the upward mandibular branches.
|
|
|
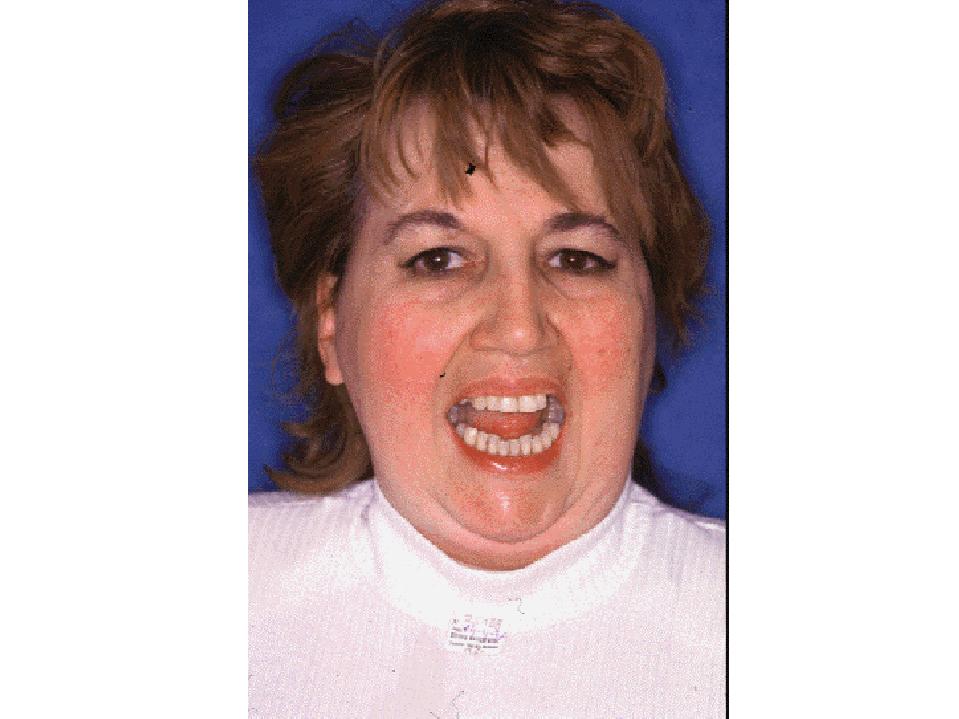
Post-treatment oral opening: 19 mm. The occlusion remains stable, with free diet, 5 years later.
|
|
Postoperative ortopantomography
Case report 2
30 years old male with postraumatic bilateral mandibular ankylosis of origin postraumático: old intracapsular bilateral fractures. The patient presented 12 mm interincisal limitation to the mouth opening, without condilar glidding movement phase.
After this surgical treatment and later rehabilitation the postoperative interincisal opening is 26 mm. Free diet. 2 years postsurgery, the mouth opening and occlusion remains stable.
|
|
|
|
|
|
|
|