PARTICIPATION
OF PATHOLOGY
IN HEALTH
CENTERS
A.- The speciality needs Technology
| INABIS '98 Home Page | Your Symposium | Related Symposia & Posters | Scientific Program | Exhibitors' Foyer | Personal Itinerary | New Search |
Impact of TECHNOLOGY in PATHOLOGY and contributions of this speciality to technological development.
Ana Maria Puras-Gil y Alfredo Lopez-Cousillas
Pathology Department. University Hospital Virgen del Camino. Navarrese Health Service - Osasunbidea.- Pamplona (Navarre). SPAIN.
E-mail: ana.puras.gil@cfnavarra.es
Impact of TECHNOLOGY in PATHOLOGY and contributions of this speciality to technological development.
|
|
"We cannot reproach our scientists for the technological explosion that is taking place in the last 100 years; however, we can try to know the effects that Science produces in our daily life, and prepare to receive its impact and learning to control it." (H. Bondi et al in Technology (3)).
The medical, chemical and biological novelties found a barrier that was dependent almost exclusively on a simple social sluggishness process..... indeed, giving up to novelties would have been either an assimilation process that they could perform with difficulty from their situation and environment, or to find themselves fired from their jobs by the new generation members that have kept updated. For that reason, the struggle around new ideas, that polemic between "old" and "modern" was mostly an encounter between generations". (J.M. López Piñero, regarding the XVII century crisis, in the Spanish Society and the Scientific Revolution (4)).
INTRODUCTION
The relationship between technological development and the medical specialty Pathology is obvious for those in direct contact with this area; but we will try to explain this relationship to those, physicians or not, with less contact with the specialty.
Anatomic Pathology or Pathology is an area dedicated to the study, by morphologic techniques and procedures (gross study, microscopy, histochemistry, immunohistochemistry, morphometric, ultrastructure, or molecular, with a different complexity according to each case needs) of the causes, development and consequences of illnesses; its ultimate aim is the correct diagnosis of biopsies, surgical specimens, cytologies and autopsies (5). It is a quite recent medical specialty in its contribution to daily Medicine practice, although historically it has been the basis of the scientific character of Medicine, and it has suffered a notable evolution (6). It is also a basic subject and so, it is of big relevance in pre- and postgraduated education, in intra- and extrahospitalary continuing medical education, and in health control; it has also a privilege place in health investigation (Table 1). A Hospital without a department of Pathology cannot be conceived.
PARTICIPATION OF PATHOLOGY IN HEALTH CENTERS
Pathology participates in Hospitals through the following areas: Diagnosis, Education, Investigation, and Hospital Information (Table 1)
The role of pathologist in the DIAGNOSIS of a disease is well know in health environment. This speciality holds the most relevant diagnosis. The study of endoscopic biopsies and surgical specimens yields almost always a definitive diagnosis; and if this is not the case, the pathologist participate in the diagnosis as a member of the "team" or in the decision-making in a clinical case. With peroperative studies, his report allows an immediate decision. Its participation in hospital o other health centers practice becomes more relevant in the diagnosis phase; but we cannot forget that it’s essential in monitorization of the evolution of transplantations and in the elaboration of protocols in the treatment of cancer or other diseases, adding information about prognosis; all this is performed through the Tumors or Tissues Commissions in the Functional Units or in Clinical Sessions.
Three fields are related with the diagnosis in Pathology are Cytology, Autopsy and Biopsy (encompassing Surgical Pathology) (Table 2). From here, Pathology executes its influence in Education and clinical investigation.
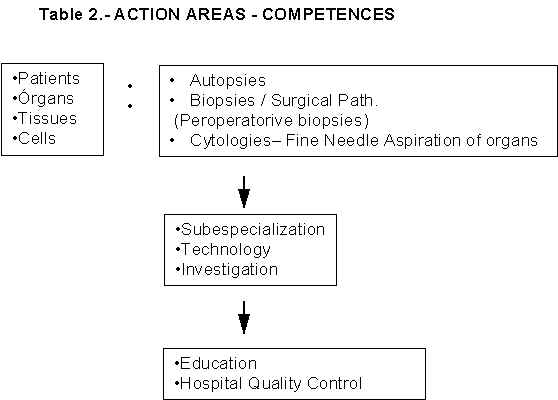
Cytology is an easy and economic method to obtain material in a patient; it deals with the study of groups of cells obtained from corporal fluids, punctures, or imprinting of organs, or from brushings; it may result in a conclusive or orientative, as well as rapid, report. The study of urine or sputum, in detection or follow up of tumors, the examination of gynecological smears in the early detection of gynecological cancer or in sexual transmission diseases, etc., make possible a quick response, not only in diagnosis, but also in the control of treatment. This is the area more related to General Practitioners.
In the last ten years the main novelties in this area of specialization has been, on one side the development of the technique of Fine-Needle Aspiration Biopsy (FNAB) where either directly or through echography or any other image control (scanner), a cellular specimen is obtained from the solid or cystic lesions, and it is effective in the diagnosis of a high percentage of lesions; on the other side, the possibility of applying immunohistochemistry, "in situ" hybridization techniques and other procedures in molecular biology to the cytological specimens, has allowed a more precise diagnosis. The specimen preparation techniques has evolved considerably, offering a notable improvement in the cytology to be studied.
Autopsy, routine, exhaustive, protocolized, and independent, taking advantage of all its possibilities, must be known in the society not only as a invaluable scientific instrument, but also as the firmest testimony of auto-criticism and medical progress (and therefore, of protection of the patient) in Hospitals and Clinical Departments.
In the White Book of Pathology, Alberto Anaya (8) points that the key to autopsy does not lie primarily on the quantity but on its purpose: in being or not part of hospital philanthropy (being in front of economical worries); making use of a proper use it should tend to constant progress in quality in attendance, following a double way of permanent intellectual improvement and recognition and solving of errors in diagnosis or treatment.
In order to fully accomplish its purposes, autopsy must be clinically informed, but it must also be independent and protocolized, and it should be performed in as great number as possible of cases, it must influence the Death Certificate, it should be used in Mortality Commission, it must be utilized in the global evaluation of the Hospital and ist Departments and every case must be discussed in Clinical-Pathological sessions
By reviewing each case with a critical spirit, it should end in a highest warranty of good performance that patients may expect from the Hospital and it will settle the basis for a free choice, with more reliable references.
The Biopsy, a specimen taken from an alive patient, or the Surgical Specimen, are oriented to obtain a diagnosis of a lesion that will de conclusive and irrevocable, regarding the nature of the disease.
The improvement in approaching techniques to obtain tissue supecimens (endoscopic biopsies, laparoscopy, etc.), and the establishment of Ambulatory Surgery are favoring the realization of quicker diagnosis by using less aggressive procedures and a closer relationship with Primary Health Centers in the area of Surgical Pathology; previously, this relationship was only present in Cytology or through Gynecology & Obstetrics speciality.
Nowadays we area dealing with more and more sophisticated methods that allow exhaustive studies of tissues, and cells too (morphometry, , immunfluorescence, immunohistochemistry, cytometry, electron microscopy...); and every time, the diagnosis must be realized with lesser amount of tissue, in more incipient tumors or diseases, or in new entities, recently appeared in the diagnosis spectrum; the first should be of help in the diagnosis difficulties of an small specimen (or even a big one) in an incipient lesion; but it is not always the case, despite the technological advances, and a fast consultation between pathologist, even from different countries, may be essential. In order to be able to carry out this we will need perfect histological sections, and only by using an adequate image transmission system we will be able to perform a fast and efficient consultation. Nowadays there is enough experience about this kind of consultations, made through computer networks (9, 10, 11, 12, 13, 14). Therefore, it is clear that technology is indispensable to reach the diagnostic aims of the speciality, as mentioned afterwards.
On the other side, we must not forget the contribution made by the pathological study to the technological, therapeutic, and diagnosis development, due to its capacity to demonstrate changes in tissues that may be due secondary to treatments, and confirming or not the its efficacy or its iatrogenia; or the possibility to compare radiological or other exploration techniques findings with the diagnosis of a lesion wholly and directly studied.
There is no doubt in the importance of the participation of pathologist in EDUCATION; although pathologists teaching the pathology course in Medical Schools need a great amount of tenacity to deal with the effects that the New Plans of Studies give rise to in the speciality, and the existence of conceptual deficiencies about the speciality at the medical practice level, the first premise maintains its validity, but it asks pathologist for a greater effort. Files, with codified pathology, the clinical-pathological Sessions with several specialities, the autopsy sessions with a clinical-pathological correlation, as well as Tumor Registries, must be used in hospital education. The Clinical-Pathological Sessions, which is the best teaching session, must be to a great extent a responsibility of the pathologist (15, 16, 17); and in order it to be carried out with success, the Hospital must give all the media needed.
Regarding INVESTIGATION, pathologist may plan several objectives classified in two different types (18), according to their orientation to themes or areas.
- Those oriented to themes, by definition, must be multidisciplinary, as it happens with health problems; the different areas must participate offering their partial knowledge, as long as this knowledge can be integrated in a whole.
- The objectives oriented to areas must power-up those scarcely developed and promptly needed to consolidate the health system. .
Ricoy (19) recommends "five principles to be followed to approach investigation in Pathology:
- Promote the generation of knowledge
- Promote the relationships between fundamental knowledge and the health problem (strategic investigation).
- Approaching the solution of specific problems that affect society, by studying them from the different points of view they influence in health, trying to find the causes and the remedies to their effects. Considering biological mechanisms, environmental factors and personal risk factors.
- Once the association between health alteration and physio-pathological mechanism in known, the methods that allow an early detection, prevention, treatment and rehabilitation must be achieved.
- Afterwards, once the investigator has established this preventive, diagnostics, therapeutic or rehabilitation procedures, he must participate in their evaluation and guarantee an appropriate utilization.
In short, by using all this mechanisms, the pathologist will influence in a decisive manner in the Hospital Quality Control, and will participate in the HOSPITAL INFORMATION. It is an alive and computerized Registry of the continuous activity in the Centers. The participation of the pathologist in Investigation, Education, Tissue, Tumors or Mortality Commissions, is essential, as weal as in other Management consultant Commissions considered by the Management of the Hospital its self.
TECHNOLOGY IN PATHOLOGY
A.- The speciality needs Technology
The microscope is the essential element in our speciality, either simple, multiple, connected to a video, to a television monitor or to a more complex device; it may have ultraviolet light, polarization prisms or any other sophisticated complement. The maximum of complexity is the electronic microscope. Electron microscopy has its biggest expansion two or three decades ago, and it has given way to other technologies that have emerged in the last ten years, but it has not lost its validity.
In order to obtain an histologic slide (Fig. 1), that is used to examine a tissue specimen under the microscope, it is necessary that the organic material goes under a series or processes; first, it is necessary to fix the tissue; to achieve this buffered formaline is used; afterwards a very this piece of tissue (a few micrometers width) is taken; to achieve the tissue must be hardened by embedding it in paraffin or freezing it. Frozen sections are generally only used in peroperative biopsies or in the detection of enzymes, hormones, some kind of reactions like antigen-antibody or in some genetic alterations. All these processes have been recently automated, not only in paraffin embedding techniques but also in fixation or staining steps. Nowadays there are automatic devices of tissue paraffin embedding for routine stainnings (Fig. 2) and for immunohistochemical studies (Fig. 3); all this have collaborated in costs saving, and with a uniformity in these techniques and a lesser contamination of specimens and of environment; considering these aspect, there are compact devices that avoid the dissemination of toxic or irritant fumes (formaline, xylol, etc.).
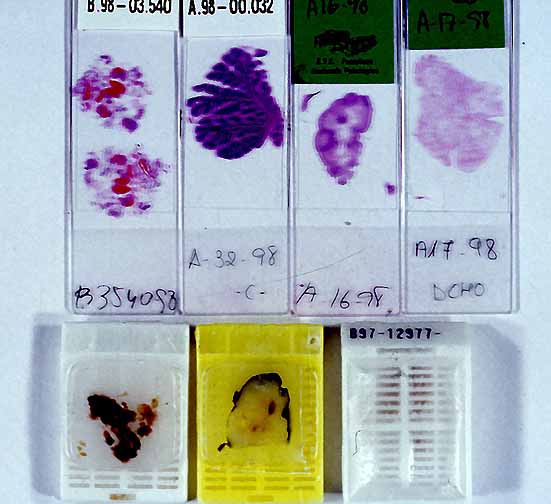 |
| Fig. 1. Paraffin blocks containing embedded tissue blocks with their
respective cassettes at the bottom. At the top, histologic slides stained with hematoxylin-eosin. |
 |
| Fig 2. Automatic staining and mounting devices of histologic slides. |
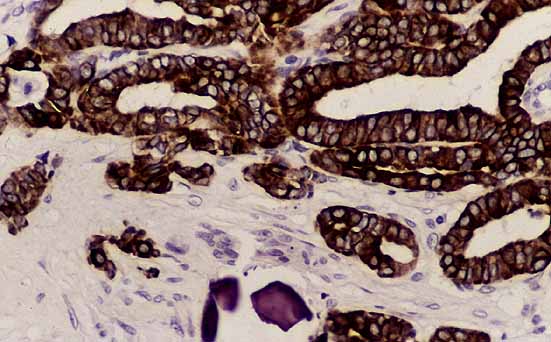 |
 Fig. 3: a) Staining device for immunohistochemical techniques. B) Adenocarcinoma with cells marked with an antibody to detect keratins (immunohistochemical technique). |
The other essential apparatus in a Pathology Department is the microtome; it is used to obtain histologic sections a few micrometers width from the paraffin embedded tissue (rotational or conventional microtome), or from the frozen tissue (cryostat) or from plastic embedded tissue for ultraestructural study (ultramicrotome)
Recently, is has also been observed a great development in automation devices for cytological diagnosis. In fact, gynecology cytology screening methods using computers are been used. New technologies have allowed the realization of in situ hybridization techniques in cellular samples for the diagnosis of viral or tumoral diseases, based in denaturalization of chromosomal DNA by heat (95º) (20), or molecular Biology techniques that are being used in the diagnosis of tumors or other diseases, Flow Cytometry (21, 22) or imaging (23, 24, 25), AgNor (26, 27), etc.
However, one of the most recent discovery is the possibility of sending digitalized images through a network (28); this can facilitate the consultation between two or more Centers. The continuing development of new technologies in this area offer the possibility of more resolution in images and a more reliable diagnosis using computer screens (29-25).
Ecography, sometimes applied in autopsies (36) or in the realization of guided fine-needle aspiration of organs, as well as radiological devices daily utilized in fetal autopsies or in osseous or calcified surgical specimens, are also used by the pathologist.
There are other tools that although less expensive are of equal importance, such as devices for automated marking of histologic slides and paraffin blocks that avoid numeration and identification mistakes, automatic saws, precision scales, paraffin dispatcher, specimens cutting tables, centrifuges, freezers, heaters, etc.
In contrast to all this machinery, the computer appears to simplify the work that can be very sophisticated in the information system and archives.
From all this, we conclude a relationship of the speciality with other areas, apparently nor connected with Medicine, but that it makes use of and to which it gives some service.
 |
 |
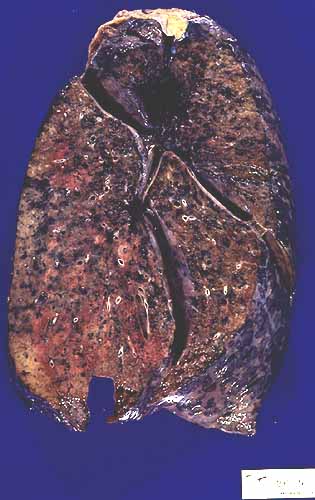
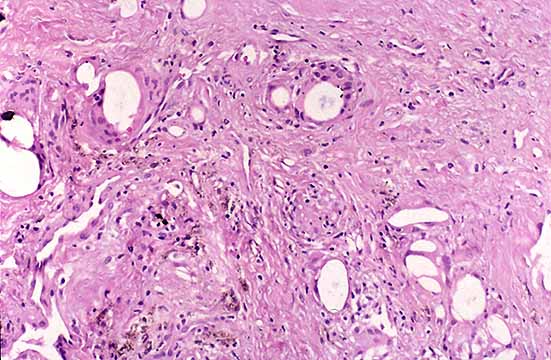
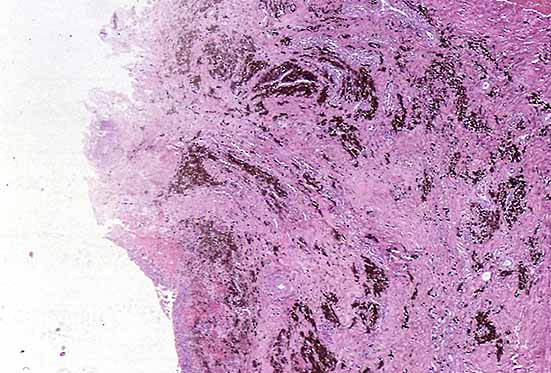
It is related to Chemistry, due to the frequent utilization of chemical products. All the tissue paraffin embedding basic procedures and the realization of histologic slides to study the tissues under the microscope area based in cellular pressure changes, dehydration-hydration and in staining chemical affinities. Histologic study also allows the detection and quantification of elements or particles, such as iron in hepatic tissue in Hemochromatosis; silica in pulmonary tissue in Silicosis (Fig. 4); copper detection, asbestos, etc. in different tissues.
 |
click to enlarge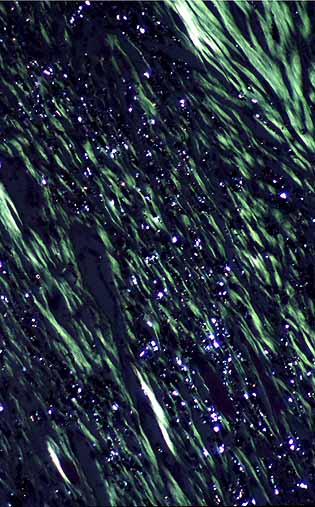 |
| Fig. 4: a) Right lung with a heavy anthracosilicosis
deposition at the right superior lobe. b) Birefringent image of silica dust in Silicosis. |
|
Generally, buffered formaline is used to fix tissues, but other fluids can be employed too, such as Bouin’s solution that permits a light decalcification in bone cylinders or fixation of meioisis in testicle biopsies, giving an adequate image of germinal cells to study infertility. There are biopsies or surgical specimens, usually bone specimens, that require decalcification if no equipment is available that allow the study without decalcification. The investigation of new chemical products is continuous (37); we need lees toxic and less irritant fixation products that don’t discolor tissues, and also decalcificants that permit a fast decalcification, preserving cell population in optimal conditions. The investigation of decalcification and demineralization procedures has facilitated the development of Paleopathology in fossils (38).
A worrisome aspect being studied is the treatment of residues originated in the Pathology Departments, either contaminant or not, to preserve the environment; some of the solutions are based in chemical reactions.
Image assisted DNA cytometry has also a cytochemical basis, the Feulgen’s reaction; it is a technique used to detect aldehyde groups generated at the cell nucleus (23).
|
 |
2.- The relationship with Physics and Mechanics can be taken from what has already been exposed. All procedures in Pathology require a perfect technology that allow the realization of thin tissue sections that are necessary for the diagnosis; this is done with a microtome, already mentioned: frozen sections (cryostat) used in peroperative biopsies, in some immunohistochemical techniques, in immunofluorescence , and in molecular biology; rotation microtomes, for paraffin embedded material, or other more specialized microtomes: to perform big sections (brain, braintome), or for non decalcified specimens (bone), or to realize semifine sections of electron microscopy studies (ultramicrotome). Automatic tissue staining devices and paraffin embedding machines, extractors, and residues transforming machines (fumes, fluids, solids), and all the machinery previously cited: centrifuges, freezers, slides and paraffin blocks markers, etc. are essential for routine work. Technology has also arrived at the transportation of specimens and pneumatic tubes are found in some hospitals for sending specimens, mainly in an urgent case like peroperative biopsy.
There is also a physical and instrumental base in DNA image Cytometry (Lambert Beer law), and also in laminar flow Cytometry (light dispersion and fluorescence): dispersed light and fluorescence signals are receives by cells that convert photons in electric pulses (39).
|
 |
The relationship with Mathematics has been established in several points: We need statistical programs in daily practice, to control costs, to realize quality controls, investigation works, publications, etc.; algorithms are used in any mathematical measurements, even in quantifying the daily practice.
Morphometry techniques, based in mathematical formulas, are used in the quantification, area and volume measurements in histological slides, where the tissue or cells are situated (40, 41); for example, to measure the depth of invasion in some skin tumors (Malignant Melanomas); to quantify percentages of germinal cells in seminiferous tubules, in the different phases of maturation, in male infertility studies (Fig. 5); to perform measurements of depth of invasion in uterine cancer, etc. (21, 40, 41).
 |
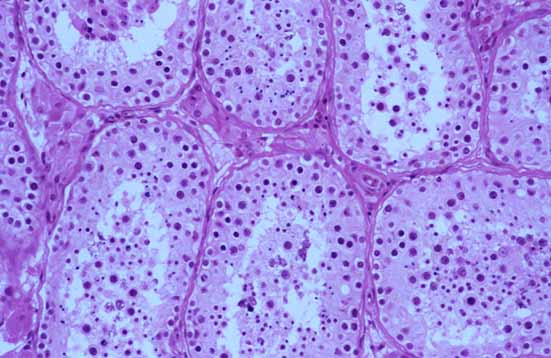 |
| Fig. 5. A) Morphometer performing a percentage quantification of
germinal cells in a testicular biopsy. B) Seminifeorus tubules being quantified. |
The automatic systems that detect nuclear changes in Cytology use coordinates in the computer to show nuclear abnormalities detected by the program; digitalized images representing a broad spectrum of abnormal cells in the smear are introduced in neural networks circuits (artificial intelligence); the objects with the highest values assigned in the neural network are selected and stored in an optical disc; afterwards, they are exposed in a high resolution video monitor; each screen can show up to 64 squares; a special software helps in the classification. This System is specially indicated in the quality Control of Cytology, or in the primary screening.
In Medical Documentation (and, therefore, also in Pathology) computer software are used and image scanners allow an uniform, clear and careful presentation in scientific presentations. (Fig. 6).
In image assisted DNA Cytometry, with diagnostic algorithms, malignancy parameters can be obtained; index and grade of malignancy, using the Böcking index. There are many related publications (21,23), since they are routinely used in many hospitals.
 Fig. 6. Inkjet Plotter used in medical Documentation. |
|
 |
4. The relationship with Telecommunication has suffered a considerable impulse in the last 5 years. An so, Telepathology is being used for consultation between Hospitals, and between them and Primary Health Center, using ISDN, alive or deferred, con static or dynamic images, and even the remote manipulation of the microscope of the consultant is already possible (42, 43). Digitalization has allowed the storing and transportation of information, Video-conferencing has been developed (44,45), Seminars, Clinical-Pathological Sessions and diagnostic consultations through networks (46-58), not only in local area networks (LAN) but also in wide area network (WAN) or Internet.
Data arrive though the network and adequate technology is all that is needed for its visualization; but can the specialist diagnose on a computer screen? This will depend on the image quality, based on the luminancy (amount of perceived) visible light, on the dynamic range (max/min perceived luminancy relation), on the noise (fluctuation luminancy with constant input), on the distortion (geometric displacement (x,y) in a pixel) (42), and in summary, on the resolution (the smallest detail that can be distinguished or measured in a visual presentation) which is dependant on the size of the point of the electron beam, on the size of the signal bandwidth and on the number of lines (raster) in the monitor in each refresh cycle (41).
There are two basic modes of transmission of multimedia data (43): a) static or "deferred": information is stored in archives for each patient or it is sent to the specialist terminal, that can reach this archive with his own access code. Undesirable accesses must be avoided, an all the necessary media must be installed to avoid sabotages and to avoid failures in confidentiality and privacy; b) interactive or alive: this is the case of alive videoconferences; this method needs a most secure, fast and potent network. One to three basic ISDN (Integrated Services Digital Network) access may be enough (2 to 6 data, voice and images lines of 64Kps).
Pregraduate education in Pathology is of easier access and understanding with the utilization of images and texts, interconnected with a computer (59, 60). These are virtual environments in teaching in Pathology; some of them (60) consist in Web pages using JavaScript to obtain a more dynamic appearance, and Java for discussion forums. It is a novel concept in distant learning because it allows instructors to create lessons or add contents in databases through Internet, and the students can reach on line this information. In Spain some universities have some experience in this mode of teaching (59, 60, 61).
In summary, Pathology expects from Engineering (that requires a theoretical knowledge of basic physics laws, mathematics, informatics, metallurgy and chemistry) that the engineer can combine such a theory with the practical appreciation of its needs. A join work must be performed to find improvements in every equipment (Hardware and Software), in communications networks (Internet, Intranet, etc.), and in documentation systems.
B.- Technology needs Pathology
The contribution of Pathology to the technological development, besides collaborating directly with professionals in the mentioned areas, exchanging information, has a direct and irreplaceable role in the application of technologies used in the diagnosis or in the treatment of diseases.
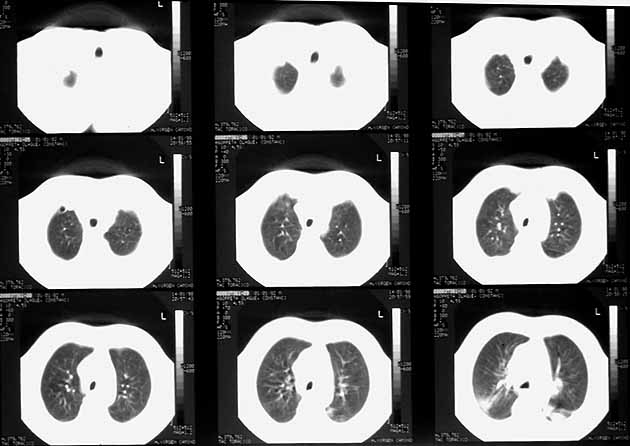
The possibility of comparing radiological or other imaging procedures, such as scanner, magnetic nuclear resonance, echography findings with the actual findings (Fig. 7) expressed in a histological slide, in the final diagnosis of the pathologist, has collaborated in a greater development of such diagnostic methods and to a greater reliability, in the continuous search of diagnostic precision.
 |
 |
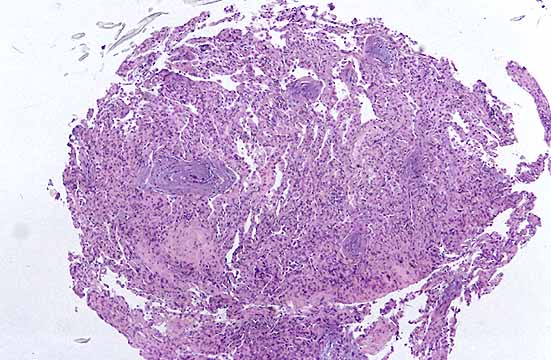 |
| Fig. 7 a) Radiological image, b) TC scanner image, and c) microscopic image of an Obliterant Bronchiolitis with Organizing Pneumonia. |
Every physician knows that the adequate joining of clinical observation, radiology, endoscopy... and the pathological diagnosis, gives Medicine a real scientific fundament.
On the other side, Pathology contributes to reassure and guide the quality of the new treatments, mainly oncologic (62), such as radiotherapy, hiperthermia, laser-therapy, or chemotherapy, showing at a tissular or cellular level the curative capacity (Fig. 8) or its iatrogenic effects. Pathological study can also show the reaction of the organism to prostheses made of different metals, plastics or porcelains (hip, breast prostheses, etc.) (Fig. 9), demonstrating the causes of rejection and the induced mechanical alterations.
click to enlarge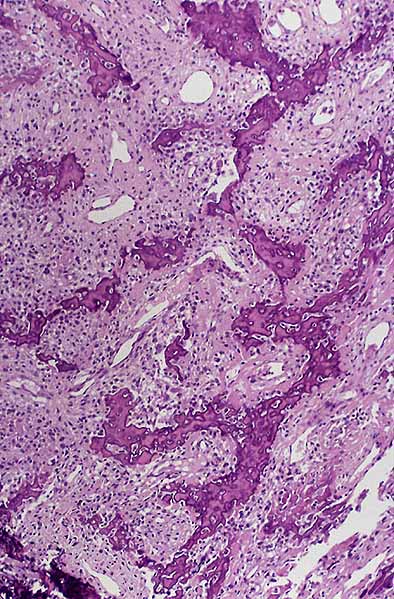 |
click to enlarge |
click to enlarge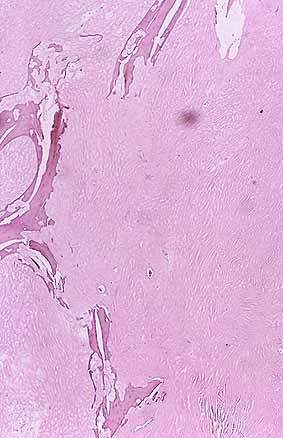 |
Fig, 8: a) Microscopic image of an osteogenic sarcoma
before any treatment. |
||
|
 |
| Fig. 9: a) Interfase rod-bone, from a prosthesis replacement, with deposits of
crystalloid pigmented material in fibrous tissue. B) Foreign body granulomatous reaction due to a crystalloid material in another case of replacement of hip prosthesis. |
ACKNOWLEDGMENTS
Thanks must be given to Thanks must be given to the Department of Electric and Electronic Engineering at the Superior Technical School of Industrial and Telecommunication Engineers of the Public University in Navarre; to Prof. Cristina Nerin, at the Superior Technical School of Industrial and Telecommunication Engineers of Zaragoza University; to the Documentation Department of the Health Department of the Navarrese Government;
We also thanks Dr. Alberto Anaya, at the Puerta de Hierro Clinic and Professor at the Autonomous University of Madrid, and to Arantza Ezpeleta, Telecommunications engineer, for her revision of the manuscript.
BIBLIOGRAPHY
1.- Ezpeleta Puras A. Analizador de Espectros por banco de filtros SC sobre Bus PC.
Proyecto Fin de Carrera. Escuela Superior de Ingenieros de Telecomunicación. Universidad
Pública de Navarra. Pamplona, Julio 1997.
2.- Spalteholz W. Vísceras, Encéfalo, Nervios, Organos de los sentidos, Vasos y Ganglios
linfáticos. En: Atlas de Anatomía Humana, III.- Edit. por Labor S.A., Barcelona, 1959.
3.- Bondi H, Bullock A, Gordon W, Piper D, Williams B. Technology. Edit por Nmarshall
Cavendish. London 1984.
4.- López Piñero JM. La Sociedad Española y la Revolución Científica. Alianza
Universidad, 1979.
5.- Vaquero M. Programa de formación en Anatomía Patológica. Comisión Nacional de la
especialidad. En: Manual del Residente en Anatomía Patológica. Hospital Univeristario
Germans Trias i Pujol. Barcelona 1997.
6.- Oliva Aldamiz H. Cajal y la Anatomía Patológica española, una Historia compartida.
Edit. por Salvat. Barcelona, 1984.
7.- Costero I. Reflexiones sobre el porvenir inmediato de la Anatomía Patológica en
España. Patología 1968; 1: 71-74.
8.- Anaya A, Menendez J, Puras A. Aprovechamiento de la Autopsia: Su importancia en el
control de calidad Hospitalario y La Autopsia del siglo XXI. Recursos calidad e impacto de
la Patología en España. Simposio Pre-congreso. XVII Congreso Nacional de la Sociedad
Española de Anatomía Patológica (Ponencia al Simposio pre-Congreso). Málaga 1997.
9.- Alfaro L, Roca MJ, Poblet E, Froufe A, Rayón M. Telepatología en Internet:
Optimización de la transmisión de imágenes con líneas de telefonía convencional.
Patología 1998; 2: 121-126.
10.- Allaert FA, Weinberg D, Dusserre P, Yvon PJ, Dusserre L, Cotran P. Evaluation of a
telepathology system between Boston (USA) and Dijon (France): glass slides versus
telediagnostic TV-monitor. Proc Annu Symp Comput Appl Med Care 1995;:596-600
11.- Brebner EM, Brebner JA, Norman JN, Brown PA, Ruddick-Bracken H, Lanphear JH.
Intercontinental postmortem studies using interactive television. J Telemed Telecare 1997;
3: 48-52
12.- Burton K, Farkas DL. Telemicroscopy. Net progress. Nature 1998 Feb 5;391:540-541.
13.- Coma del Corral MJ, Martín A, Da Costa AR, Attourah MH, Serrano I. Integración de
Recursos Telemáticos: UniNet y la Comunicación en directo. II Congreso Virtual
Hispanoamericano de Anatomía Patológica. (Junio 1998)
14.- Dunn BE, Almagro UA, Choi H, Sheth NK, Arnold JS, Recla DL, Krupinski EA, Graham AR,
Weinstein RS. Dynamic-robotic telepathology: Department of Veterans Affairs feasibility
study. Hum Pathol 1997 Jan;28(1):8-12
15.- Oliva H, Pardo-Mindan FJ. Estructura básica de la formación Anatomopatológica.
Enseñanza de la Patología con apoyo informático. Recursos calidad e impacto de la
Patología en España. Simposio Pre-Congreso. XVII Congreso Nacional de la Sociedad
Española de Anatomía Patológica. Málaga, 1997.
16.- Ortuño G, Pastor F, Martinez Díaz F, Vicente V, Blasco P. Problemática profesional
y jurídico-laboral. Recursos calidad e impacto de la Patología en España. Simposio
Pre-Congreso. XVII Congreso Nacional de la Sociedad Española de Anatomía Patológica.
Málaga, 4-8 Oct, 1997.
17.- Toledo JD, Herrero A. Estandarización de informes en Anatomía Patológica. Recursos
calidad e impacto de la Patología en España. Simposio Pre-Congreso. XVII Congreso
Nacional de la Sociedad Española de Anatomía Patológica. Málaga, 4-8 Oct, 1997.
18.- Nogales F, Hierro I, Alvarez M. La Investigación en Patología. Recursos calidad e
impacto de la Patología en España. Simposio Pre-Congreso. XVII Congreso Nacional de la
Sociedad Española de Anatomía Patológica. Málaga, 1997.
19.- Ricoy JR. Simposio Pre-Congreso. Congreso Nacional de la Sociedad Española de
Anatomía Patológica. Barcelona 1995.
20.- Lleonart M E , Sánchez R , Martín-Duque P y Ramón y Cajal S . Técnicas de
hibridación, donación y secuenciación de ácidos nucléicos en el diagnóstico
anatomopatológico. Rev. Esp. Patol 1997; 30: 249-257.
21.- Pimenova EL, Sheremet'eva GF, Bogatyrev VN. Use of morphometry and DNA flow cytometry
in the differential diagnosis, prognosis and treatment of primary tumors of the liver.
Klin Lab Diagn 1996 ;2:7-11
22.- Sanz-Ortega J, Sanz-Esponera J, López JA. Valor pronóstico de la ploidía
determinada mediante citometría de flujo en el cáncer gástrico. Rev Esp Pat 1995; 28:
95-100.
23.- Sampedro A , Hardisson D A , Martínez-Nistal A y Urdiales G L . Citometría de ADN
asistido por imagen. En: Bases de la Proliferación Celular y su Aplicación en la
Práctica Clínica. - Cap. 10, 1984: 169-199. Edit. por Universidad de Oviedo.
24.- Toledano A. Requerimientos metodológicos para el óptimo aprovechamiento del
análisis de imagen automatizado y el futuro de esta técnica. Patología 1996; 29:
377-378.
25.- Corcuera Pindado MT, Gómez Aguado A, Picazo Talavera A, Roldán-Contreras M,
Alonso-Martín MJ. Aplicación del análisis de imágen para cuantificación de la
actividad NADPH-DH en axones de la capa molecular de cerebelos de rata tratados con AZT.
Patología 1996; 29: 373-375.
26.- Gimenez-Mas JA, Gallego-Calvo P, Sanz-Moncasi P, Rios-Mitchell J, Valero I,
Sanz-Anquela M, Burriel J, Bavai A. AgNOR evaluation by image processing methods. Staining
modifications and results in 126 invasive ductal breast carcinomas. Anal Quant Cytol
Histol 1996 Feb;18(1):9-18
27.- Gimenez-Más JA, Sanz-Moncasi MP, Remon L, Gambo P, Gallego-Calvo MP. Automated
textural analysis of nuclear chromatin. A mathematical morphology approach. Analyt Quant
Cytol Histol 1995; 17: 39-47
28.- Martinez-Nistal A y Sampedro A . Introducción al proceso digital de imágenes. En:
Técnicas de Fluorescencia en Microscopía y Citometría, 1984: 31-47. Edit. por
Universidad de Oviedo.
29.- Weinstein MH, Epstein JI. Telepathology diagnosis of prostate needle biopsies. Hum Pathol 1997; 28: 22-29.
30.- Galvez J, Howell L, Costa MJ, Davis. Diagnostic concordance of telecytology and
conventional cytology for evaluating breast aspirates. Acta Cytol 1998 May;42(3):663-667.
31.- Pimenova EL, Sheremet’eva GF, Steffen B, Gianom D, Winkler C, Hosch HJ,
Oberholzer M, Famos M. Frozen section diagnosis using telepathology. Swiss Surg
1997;3(1):25-29
32.- Allaert FA, Weinberg D, Dusserre P, Yvon PJ, Dusserre L, Cotran P. Evaluation of a
telepathology system between Boston (USA) and Dijon (France): glass slides versus
telediagnostic TV-monitor. Proc Annu Symp Comput Appl Med Care 1995; 18: 596-600
33.- Ferrer Roca O . Immunohistochemical correlation of esteroid receptors with disease
free interval in 206 consecutive breast cancers. Validation of the telequantification
based on global scene segmentation. Anal Cell Pathol 1995; 9: 151-163.
34.- Garcia-Bonafe M, Moragas A. Differential diagnosis of malignant and reactive cells
from serous effusions: image and texture analysis study. Anal Cell Pathol 1996
Nov;12:85-98.
35.- Cochran A J , Bailly C , Cook M, Crotty K and als, Recomendations for the reporting
of tissues removed as part of the surgical treatment of cutaneous melanoma. Rev. Esp.
Patol. 1997; 30: 69-71.
36.- Fariña J. La Ecografía en los Estudios Postmortem: Ecopsia. II Congreso Virtual
Hispano-Americano de Anatomía Patológica. (Junio 1998)
37.- Muñiz, E, Rodriguez-Mateo L, Martinez Rodriguez R, Gragera RR. COMPLUCAD: un nuevo
fijador para muestras histopatotógicas. II Congreso Virtual Hispano-Americano de
Anatomía Patológica. (Junio 1998)
38.- Tamarit- Montesinos L. Comunicación personal.
39.- Toyos J , Salas A y Sampedro A . Bases instrumentales de la Citometría de flujo. En:
Técnicas de Fluorescencia en Microscopía y Citometría, 1984: 191-208. Edit. por
Universidad de Oviedo. -
40.- Hamilton PW, Allen DC. Morphometry in histopathology. J Pathol 1995; 175: 369-379
41.- Moragas A, Garcia-Bonafe M, de Torres I, Sans M. Textural analysis of lymphoid cells
in serous effusions. A mathematical morphologic approach. Anal Quant Cytol Histol 1993
Jun;15(3):165-170
42.- Telefónica I+D. Telemedicina. Comunicación personal.- Madrid, 1.996.
43.- Vaamonde Lemos R. Telemedicina y Telepatología (Desarrollo y Aplicaciones)
Conferencia en el II Congreso Virtual Hispano-Americano de Anatomía Patológica. (Junio
1998)
44.- Ferrer Roca O. Videophone in pathology: interactive DNA and immunohistochemical
measurements betwen European countries. Patología 1991; 24: 225-229.
45.- Ferrer Roca O . Narrow and Broad Band Communications. VHS-video DL-Tf361/1994. Spain:
Catai Assoc.
46.- Ferrer O , Pitti S , Diez Cardama A and als. Factors influencing distant
tele-evaluation in citology, Pathology, conventional Radiology and Mammography. Analytical
Cellular Pathology 1996; 10: 13-23.
47.- García-Rojo M, Sánchez Ramos M. Internet. Boletin informativo de SEAP 1996; 13:
2-3.
48.- Ferrer Roca O , Díaz Cardama A , Pitti S , Ramos A , Gómez E , Tejera A , Spencer J
. Telemedicine in teh Canary Islands. Lancet 1995; 345: 1177-1178
49.- Calles P W , Leslie K O , Mattia A R , Weaver D L and als. Diagnostic accuracy of a
rural live video Telepathology system. Am J Surg Pathol. 1997; 21:812-819.
50.- Allaert FA, Weinberg D, Dusserre P, Yvon PJ, Dusserre L, Retaillau B, Cotran P.
Evaluation of an international telepathology system between Boston (USA) and Dijon: glass
slides versus telediagnostic television monitor. J Telemed Telecare 1996;2 Suppl 1:27-30
51.- Dervan PA, Wootton R. Diagnostic telepathology. Histopathology 1998 Mar;32(3):195-198
51.- Martinez Nistal A, Sampedro A, Secades C. Búsqueda e intercambio de información en
Anatomía Patológica a través de Internet. Patología 1995; 28: 403-408.
52.- Della Mea V, Forti S, Puglisi F, Bellutta P, Finato N, Dalla Palma P, Mauri F,
Beltrami C. Telepathology using Internet multimedia electronic mail: remote consultation
on gastrointestinal pathology. J Telemed Telecare 1996;2(1):28-34
53.- Raab SS, Robinson RA, Snider TE, McDaniel HL, Sigman JD, Leigh CJ, Thomas PA.
Telepathologic review: utility, diagnostic accuracy, and interobserver variability on a
difficult case consultation service. Mod Pathol 1997 Jun;10(6):630-635
54.- Brebner EM, Brebner JA, Norman JN, Brown PA, Ruddick-Bracken H, Lanphear JH.
Intercontinental postmortem studies using interactive television.J Telemed Telecare 1997;
3: 48-52
55.- Weinstein LJ, Epstein JI, Edlow D, Westra WH. Static image analysis of skin
specimens: the application of telepathology to frozen section evaluation. Hum Pathol 1997
Jan;28(1):30-35
56.- Weinstein MH, Epstein JI. Telepathology diagnosis of prostrate needle biopsies. Hum
Pathol 1997 Jan;28(1):22-29
.
57.- Weinstein RS, Bhattacharyya AK, Graham AR, Davis JR Hum Pathol 1997 Jan;28(1):1-7.
Telepathology: a ten-year progress report.
58.- Gombas P, Szende B, Stotz G. Support by telecommunication of decisions in diagnostic
pathology. Experience with the first telepathology system in Hungary. Orv Hetil 1996 Oct
20;137(42):2299-2303
59.- Pardo J. Programa informático de docencia en Anatomía Patológica INTERPAT. Edit
por Mosby. Madrid 1997.
60.- Sampedro A, Rubio R, Pavón A, Suárez D, Gimeno AS, Del Cura Y, Nistal AM. WELLPATH.
Entorno Virtual para la formación en Anatomía Patológica. Conferencia en el II Congreso
Virtual Hispano-Americano de Anatomía Patológica. (Junio 1998)
61.- Pavon A Y , Secades C , Martínez-Nistal A y Sampedro A . Sesiones
clinicopatológicas interactivas en Internet. Int. Telemedicinal 1997; 4: 40-44.
62.-Becker W. Definición y lugar de la Patología: Editorial. Patología 1987; 20:
147-149.
| Discussion Board | Previous Page | Your Symposium |