|
|
Oral & Maxillofacial Service Hospital Universitario "Del Río Hortega" Valladolid. SPAIN |
|
| INABIS '98 Home Page | Your Poster Session | Related Symposia & Posters | Plenary Sessions | Exhibitors' Foyer | Personal Itinerary | New Search |
|
|
Oral & Maxillofacial Service Hospital Universitario "Del Río Hortega" Valladolid. SPAIN |
|
MICROSURGICAL RECONSTRUCTION OF PERIPHERIC FACIAL NERVE BY MEANS GREATER AURICULAR NERVE GRAFT
Garcia Cantera, JM
, MD, PhD; Perez Gonzalez, E*, MD, Phd; Blanco Rueda, JA, MD, PhD; Izquierdo Millan, M, MD; Garcia Reija, F, MD; Verrier Hernández, A, MD, PhD.Oral & Maxillofacial Surgery Service.
(*) Radiology Service.
Hospital Universitario Rio Hortega.
Valladolid. SPAIN
Contact person:
J.M.García Cantera. e-mail: mcantera@lander.es
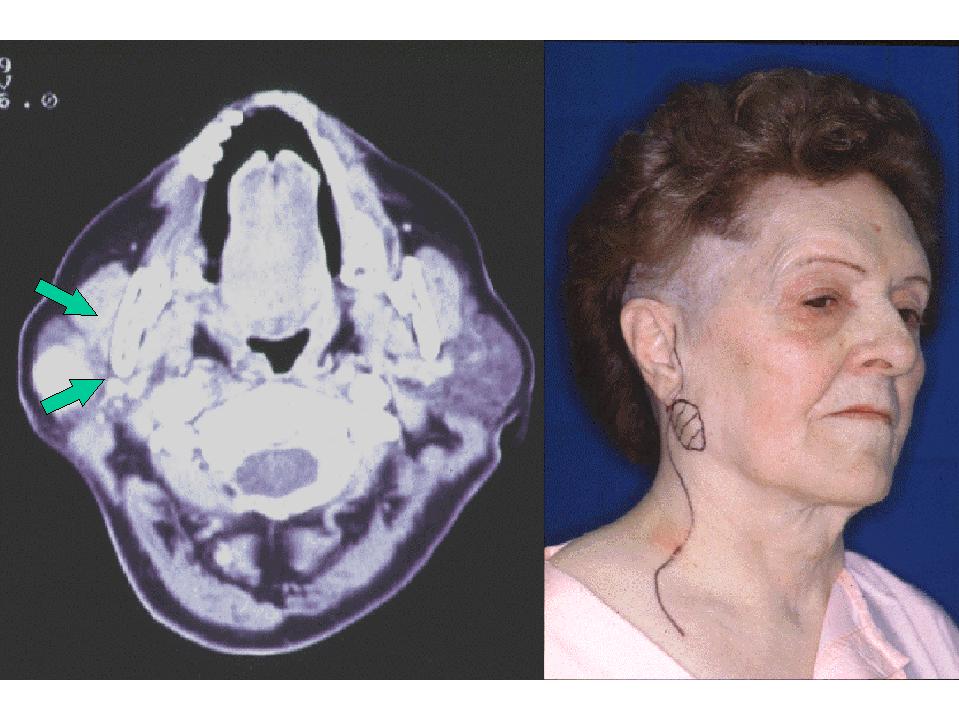
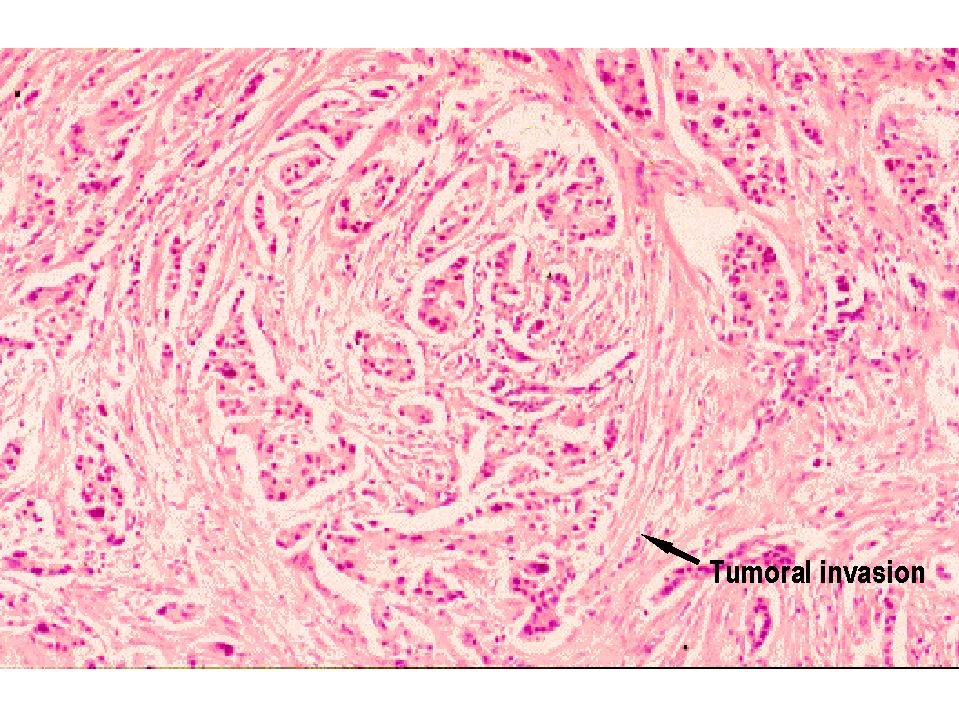
We present a case of parotid gland adenocarcinoma (high degree malignancy) in right parotid area of 3 cm diameter, stuck to skin and deep planes.
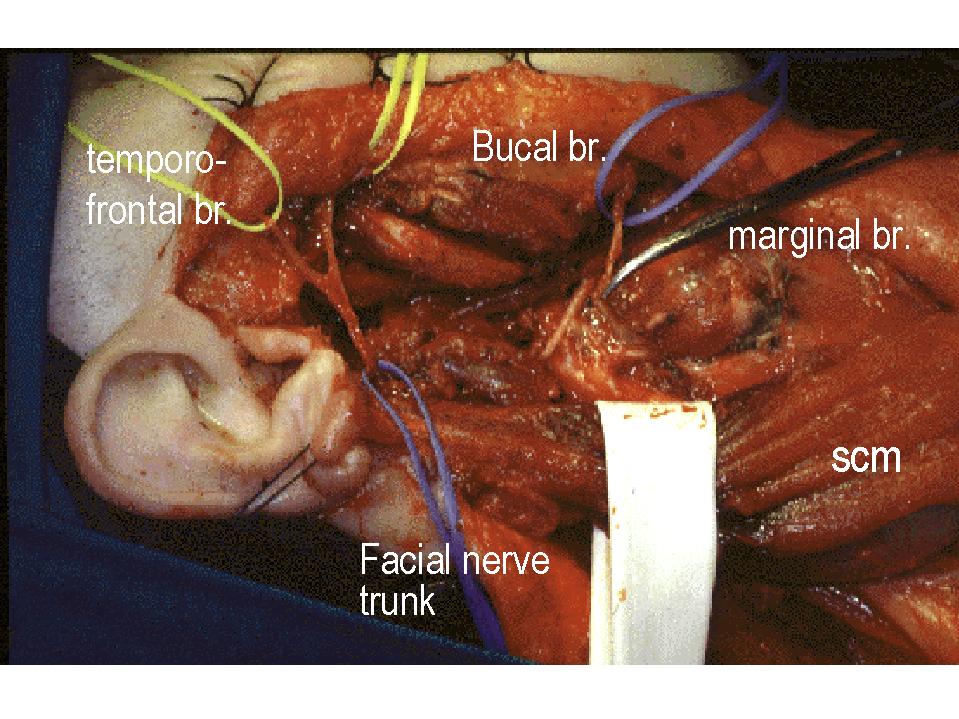
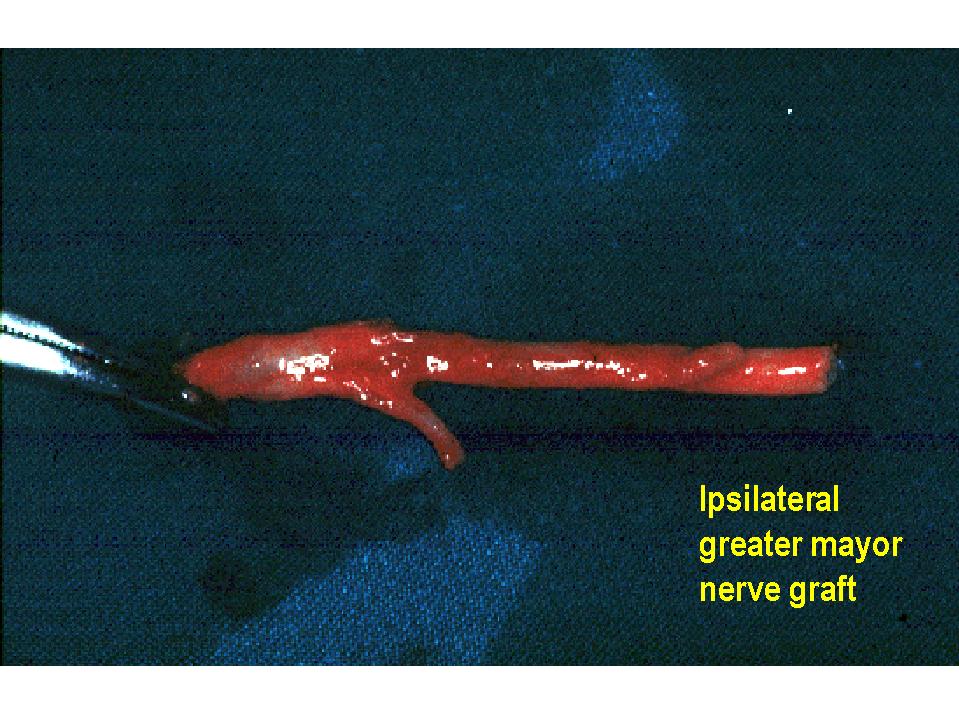
We practice radical parotidectomy with resection of the affects cutaneous area and functional cervical homolateral dissection. When existing it only intraoperatory evidence of tumoral invasion of the facial marginal nerve, we have preserved the frontal and buccal branches. The marginal branch is reconstructed by means of an 2,5 cm lenght greater auricular nerve graft. Cutaneous traslation–rotation cervical flap was made.
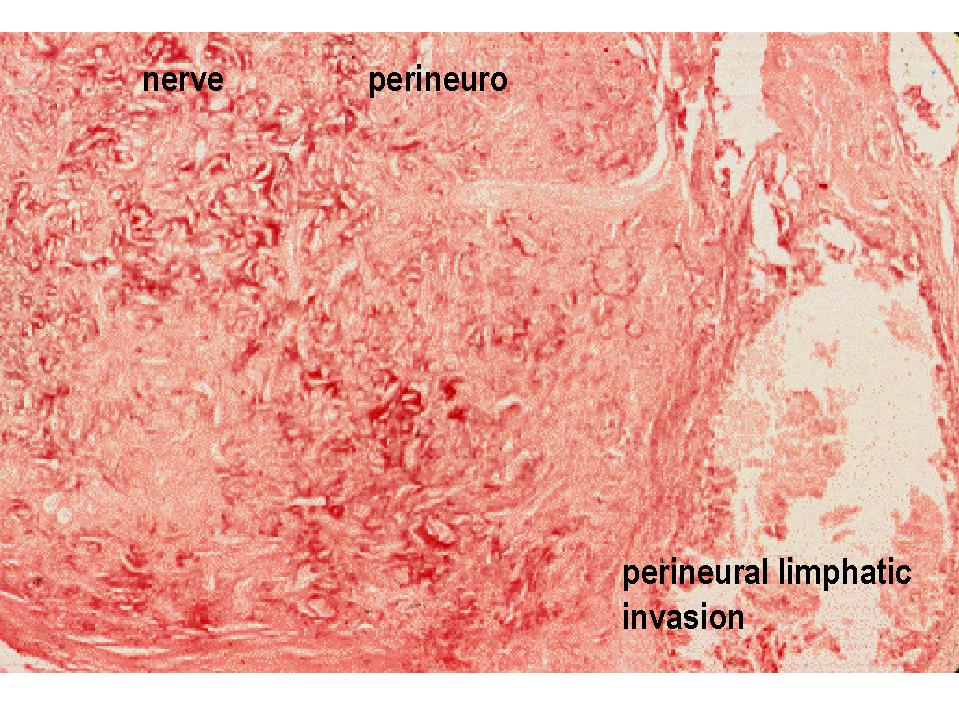
The postoperative pathologic study shows high degree parotid gland adenocarcinoma with cutaneous and marginal nerve invasion. Two superior cervical group metastic ganglions. Postoperative chemotherapy was practiced.
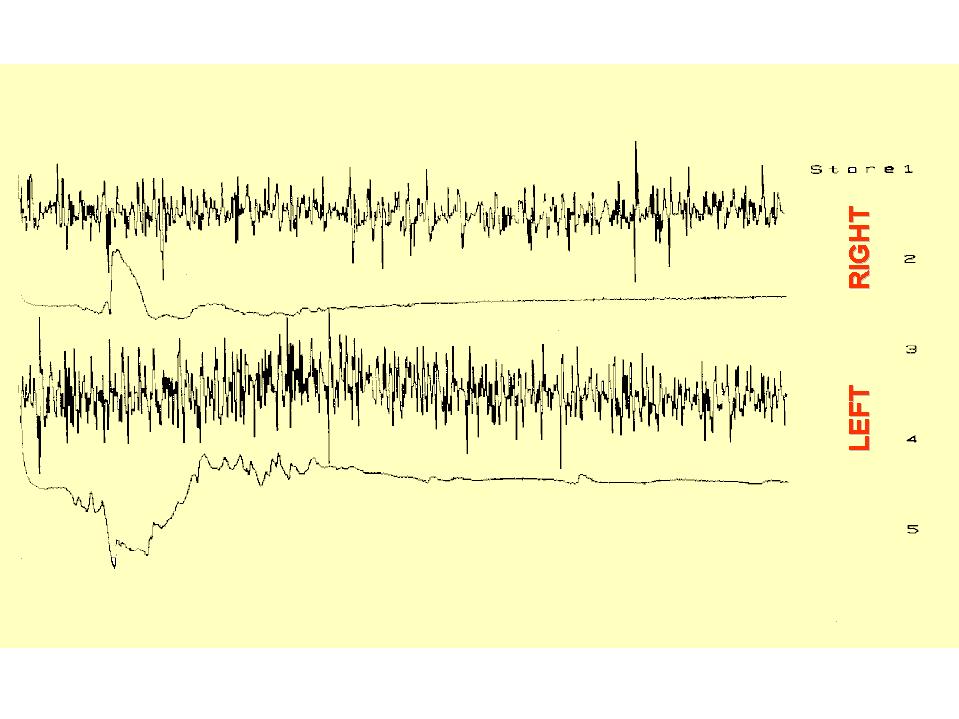
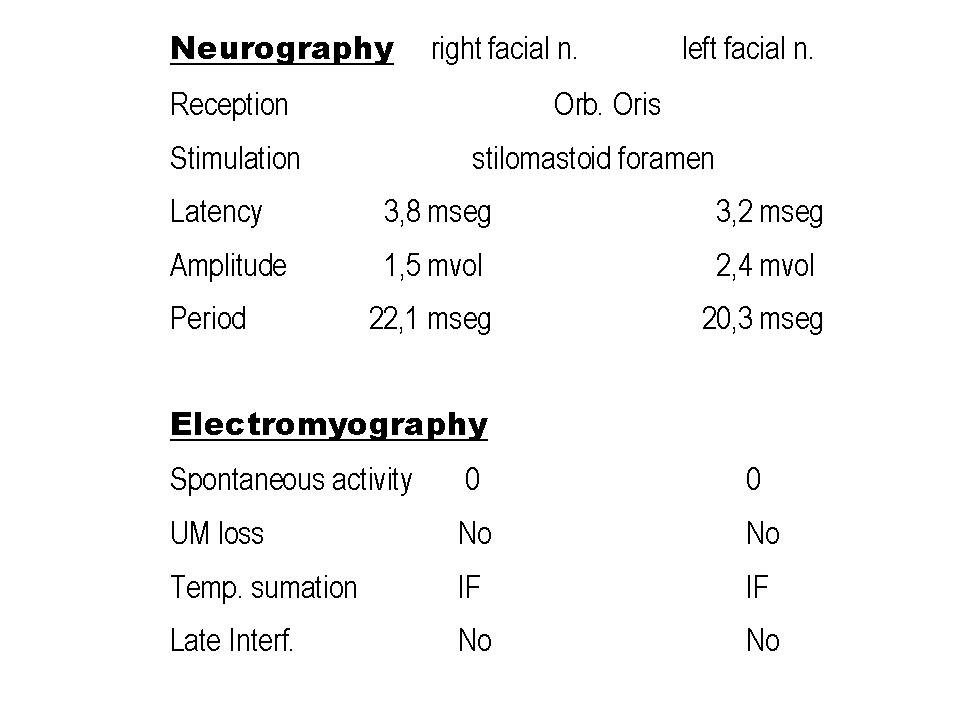
To the 5 years postsurgery the patient is free of relapse. The clinical, miographic and neurographic explorations are inside the normality levels in comparison with the healthy side.
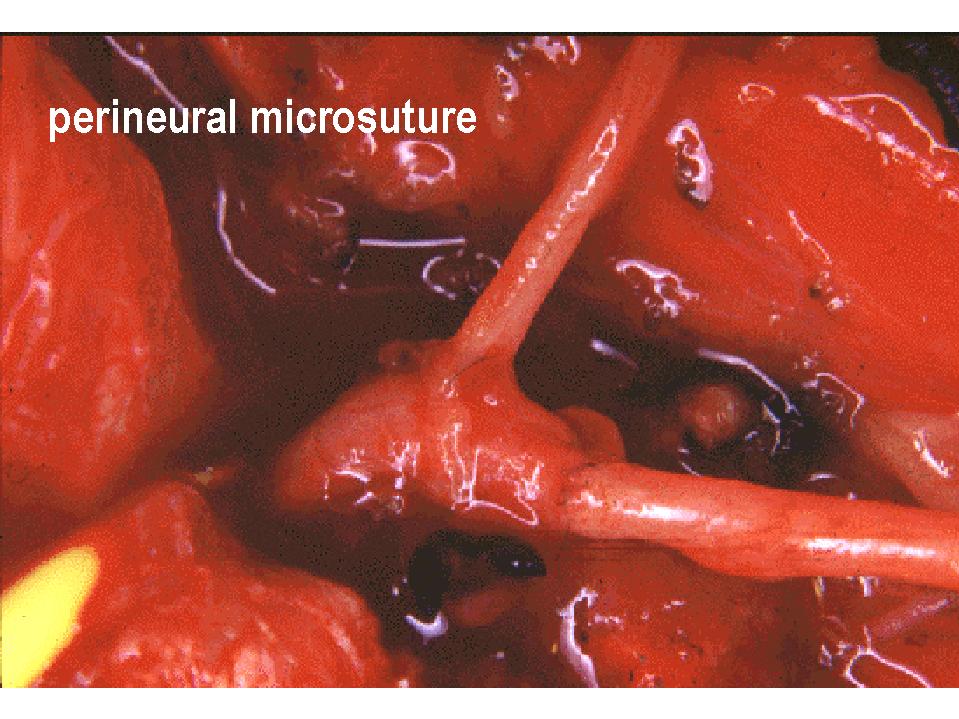
One of the challenges in reconstructive surgery is the repair from the substance losses to level of the pheripheric nerves. To get the confrontation of both nervous ends, the substance loss forces to carry out it microsuture under tension that is the main cause of failure of the same one, for different reasons:
Lundborg (1975) estimate that the critical interval starting from which term-terminal microsuture is non-viable because of the alteration of the nervous vascularization that produces the tension of the suture focus in 8% of the overall length of the nerve.
To solve this problem, different resources have been used, as placing the extremity in flexion, nervous traspositions, bony fragments resection to shorten the extremity affects, filament guides, tubulizations, etc. At the present time the election technique is the use of nerve autogenous grafts. In this publication we present a easy technique for the reconstruction of substance losses at level of the facial nerve.
|
|
76 years old female patient that goes to consultation to present three months slowly progressive growth evolution hard mass at level of right parotid area of 3 cm diameter, stuck to skin and deep planes. Clinically no cervical loco-regional metastic ganglions. Absence of facial paresis.
|
|
|
|
|
|
|
The fine needle punction-aspiration suggests diagnosis of high degree malignancy parotid gland adenocarcinoma.
We practice radical parotidectomy with affects cutaneous area extirpation and functional cervical dissection, as well as microsurgical nervous defect reconstruction by means ipsilateral greater auricular nerve graft (2 cm) and close by means advance-rotation cutaneous flap. When only existing intraoperatory marginal branch affectation, we decides to preserve the frontal and buccal facial branches.
|
|
|
The anatomo-pathological study shows high degree malignancy parotid gland adenocarcinoma with cutaneous and marginal nerve invasion. Two metastatic superior cervical ganglions group. 19 marked sinusal histiocytosis ganglions. She was carried out postoperative chemotherapy. (Hematoxylin-eosin staining).
|
|
5 years postsurgery, the patient is free of relapse. The clinical, myographyc and neurographyc explorations are inside the normality in comparison with the healthy side.
|
|
|
|
Discussion Board | Previous Page | Poster Session |