Neuroscience Poster Session
| INABIS '98 Home Page | Your Session | Symposia & Poster Sessions | Plenary Sessions | Exhibitors' Foyer | Personal Itinerary | New Search |
Introduction
Introduction:
The nervous system constantly adapts to environmental changes by quickly adjusting motor commands to make accurate movements. Such adjustments occur, for example, when lifting a kettle that is unexpectedly empty. Other examples of such behavior include corrections during pointing movements in response to shifted visual targets (Flanagan et al. 1993; Flash & Henis 1991; Van Sonderen and Denier van der Gon 1990), responses to Coriolis force pertubations produced in a rotating room (Lackner & Dizio 1994), and responses to artificially generated velocity-dependent (Shadmehr & Mussa-Ivaldi 1994) or position-dependent force perturbations (Feldman 1966; Feldman & Levin 1995; Weeks et al. 1996). In particular, in a study by Weeks et al. (1996), subjects produced fast non-obstructed elbow movements to a target and, starting from a randomly selected trial, the movements were opposed by a spring-like load. In the first movement against the load, subjects made an error requiring correction. However, after the first trial, subjects made subsequent movements against the load directly to the target without corrections. The patterns of errors and the rapid adjustments of the movements to new load conditions were well explained in the framework of the l model of motor control (Feldman & Levin 1995). This model suggests that the nervous system memorizes the central commands established after corrections in the first trial with the new load and reproduces them in the next and subsequent trials. The ability of the damaged central nervous system (CNS) to process and adapt movement to new load conditions is unknown. CNS lesions in the brain result in sensorimotor deficits including spasticity, muscle weakness and hemiparesis, or movement deficits of the contralateral hemicorps. The rehabilitation of hemiparetic patients is broadly based on movement repetition in order to learn new motor patterns. Two processes may be involved in motor learning: the ability to modify the motor command as a function of variations in the external environment and, the capacity to integrate previously acquired skills into motor performance. These may be expressed by the specification of an adequate central command and by the use of short-term memory.
The goals of this study were to identify the correction strategies used by hemiparetic subjects during elbow flexion movements and to compare them with those used by healthy subjects. The further understanding of error correction mechanisms in healthy subjects as well as deficits in central commands in patients with CNS lesions may lead to the development of more effective rehabilitation techniques to optimize sensorimotor recovery processes and improve functional ability in these patients.
Materials and Methods
Methods:
Ten hemiparetic subjects aged less than 70 years old participated in this study approved by the Ethics Committee of the Institut de r�adaptation de Montr�al. They had sustained a stroke between 3 months and 3 years previously and had moderate to mild motor deficits in the affected arm (Chedoke-McMaster Arm Function Score > 3). As can be seen in Figure 1,
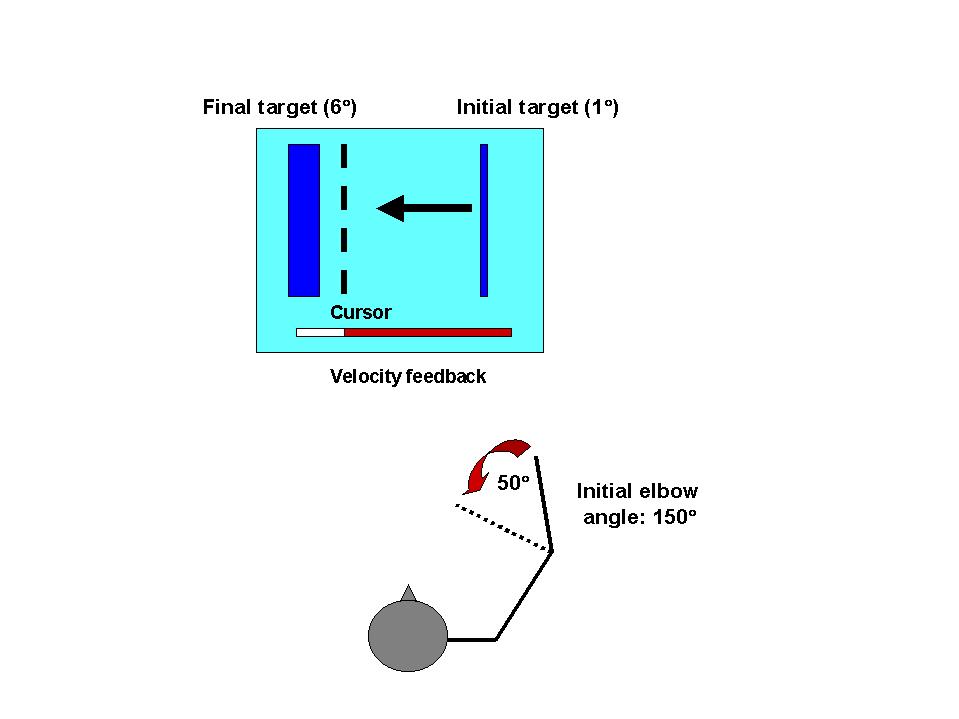 Fig. 1:experimental setup.
Fig. 1:experimental setup.
subjects were seated in a chair with the right forearm supported on a horizontal manipulandum and the flexion/extension axis of the elbow aligned with the axis of rotation of the shaft of the torque motor (for details see Feldman et al. 1995). The seat was adjusted so that the initial position of the shoulder corresponded to 30� flexion and 45� abduction. The wrist was immobilized by a polypropylene splint in the neutral position for the entire experiment. The arm position ensured that the subject would easily be able to perform isolated single degree-of -freedom movement of the elbow. Subjects were required to make a single 50� elbow flexion movement from an initial position (150� extension with full extension being defined as 180�), to a final position.
During the experiment, the subjects had visual feedback on a computer screen on which the starting position and the final target were represented by a 1� and a 6� window respectively. The hand position was indicated by a cursor which the subjects moved from the initial to the final target by a single elbow flexion. They were instructed to move "as fast as possible" on all trials. They were also instructed not to correct (control trials) or to correct (experimental trials) movement errors resulting from the sudden introduction of an external load produced by a torque motor. The appropriate load was chosen as a function of the subject's maximal strength. The load was produced by a torque motor that was attached to the manipulandum. For movement with the load, the load was zero at the initial position and increased as a linear function of arm displacement to the target (spring-like-load). It was applied for a series of 5 to 10 trials, then removed for the next series of 5 to 10 and then series were alternated for a total of approximately 120 trials. The number of trials for each condition was chosen randomly to prevent subjects from anticipating the change in load and making preparatory adjustments. The subject first had to train for 30 to 60 trials without the load. The goal of the training session was to familiarise the patient with the apparatus and to practice making both fast and accurate movements Angular position and velocity data along with torque and electromyographic activity from 4 muscles (2 elbow flexors and 2 elbow extensors) were recorded. Movement precision, movement duration and velocities were recorded.
Trials were individually analyzed on an interactive video display to determine the initial position, the peak velocity, the onset of movement (which corresponded to the position at which velocity exceeded 10% of the peak velocity), the steady-state torque in the final position, the final position before correction and the final position after correction. The final position was determined by the combination of information provided by the velocity/time (Fig. 2A), the position/time (Fig. 2B) and the velocity/angle (Fig. 2C) graphs as shown in Figs.2 and 3.
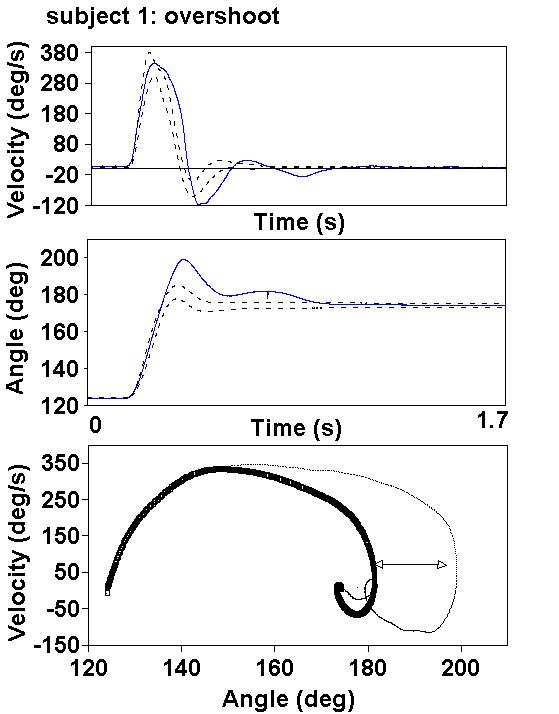 Fig. 2:subject 1: overshoot.
Fig. 2:subject 1: overshoot.
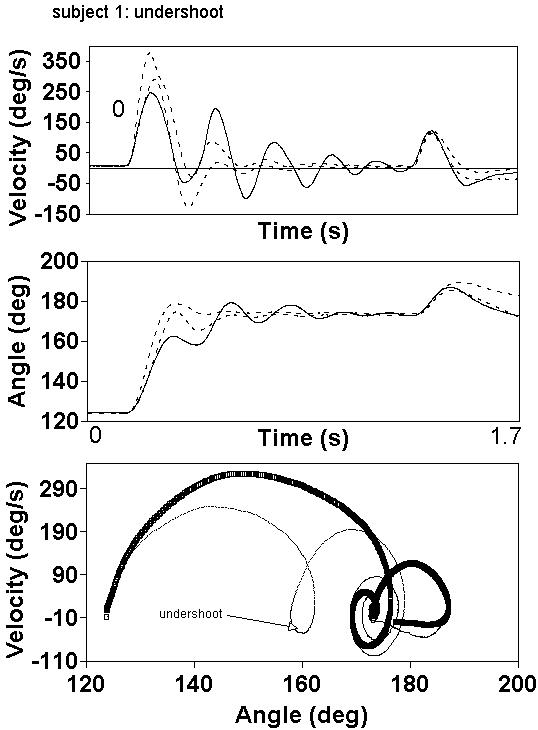 Fig. 3:subject 1: undershoot.
Fig. 3:subject 1: undershoot.
Data in Figs. 2 and 3 is from a subject with mild (S1) motor dysfunction. In Fig. 2A, B the continuous line is an example of a corrected trial and the dotted lines are averages of the movement made under the same load conditions but without correction. The final position before correction (arrow) and the corrective movement to reach the target can clearly be seen in the velocity/angle diagrams (Figs. 2C and 3C). In figure 2 the subject is doing an overshoot when the load condition is changing from with load to no load and in figure 3 the subject makes an undershoot when the load condition changes from no load to with load (for more details on analysis methods see Weeks and al. 1996). Note that, for this analysis, we determined only the final positions before correction since this position is the only one that reflects the initial central command specified by the subject before the onset of the movement.
Results
Results:
Final elbow positions before corrections for all trials in a subject with a mild hemiparesis (Subject 1) are shown in Fig. 4.
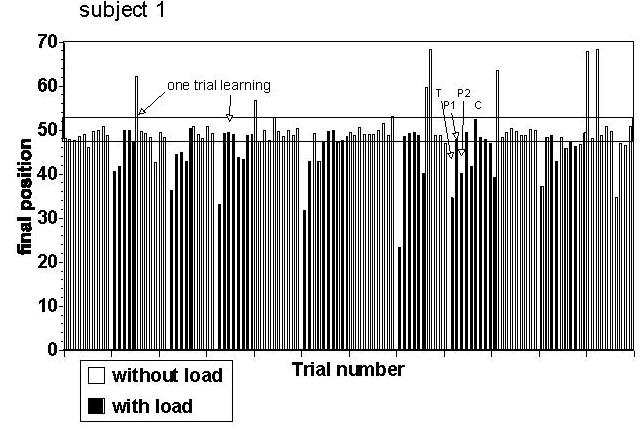 Fig. 4:Final position for subject 1.
Fig. 4:Final position for subject 1.
The test trial (T) was the first trial in which the subject's arm encountered changed load conditions. Trials P1 and P2 are the second and third post-test trials respectively after the load condition changed. All other trials in the same load conditions are classified as C or control trials.
Using the same experimental paradigm in a healthy group of subjects, Weeks et al. (1996) described that in the T trials, subjects either undershot (when load conditions changed from "no load" to "load") or overshot the target (when conditions changed from "load" to "no load"). Correction of the error mainly occurred in the P1 and P2 post-test trials. They identified four error correction patterns based on final positions in T, P1 and P2 trials after the introduction or removal of the external load. All of these patterns resulted in the correction of the error in the T trial in less then 3 trials. The most frequent pattern was one in which the error in final position in the T trial was corrected in the first post-test trial (P1). This pattern described a process of one-trial learning (arrow).
Most of the hemiparetic subjects with mild sensorimotor deficits behaved similarly to the healthy subjects in terms of the error observed in the T trials and the corrections within the subsequent 2-3 trials. In subjects with severe sensorimotor deficits however, no stable correction patterns were identified (Fig. 5).
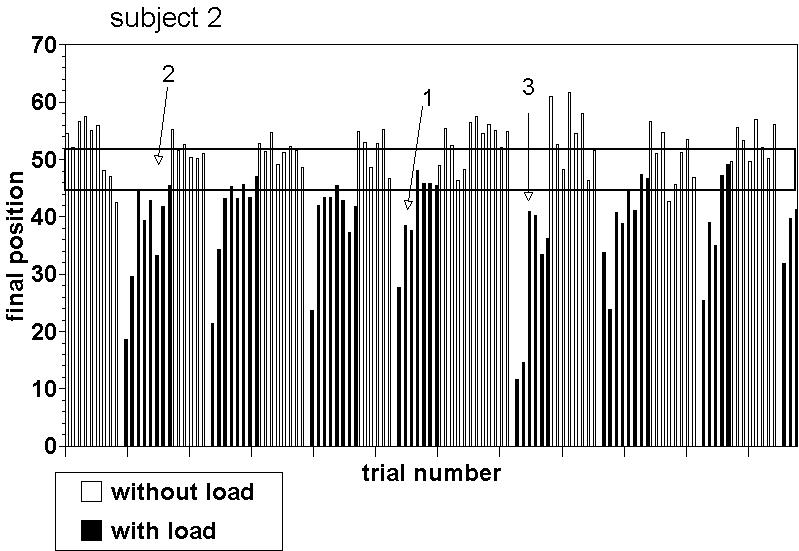 Fig.5: Final position for subject 2.
Fig.5: Final position for subject 2.
Corrections were often made after more than 3 trials (arrow #1). In these subjects, even when the target was reached in fewer than 3 trials, the behavior was not stable and consistent, accurate movement was not produced during the subsequent like-load C trials (arrow #2).In some blocks, subjects failed to make accurate movements in all of the C trials of the same load condition (arrow #3).
The average peak speed of elbow flexion was < 400�/s for all the hemiparetic subjects, which was significantly lower than that for normal subjects (554�/s: from Weeks et al. 1996). Thus, it was possible that undetected "on-line" corrections occurred in the hemiparetic subjects. However, in a control experiment in which 3 healthy subjects were trained to perform the task at speeds less than 400�/s, movement errors and correction patterns were similar to those observed when subjects were asked to move "as fast as possible". Thus, it is unlikely that differences in behavior between hemiparetic and healthy subjects were due to differences in movement speed.
Averages and standard deviations of final positions for each type of trial under the two external load conditions were calculated for all subjects. The behavior of some subjects did not differ from that in healthy subjects. For Subject 1 (Fig. 5) errors were corrected in fewer than 3 trials 67% of the time when load conditions changed from no-load to with-load and 71% of the time for the load changes in the opposite direction. In general, two subjects with mild impairments behaved similarly to healthy subjects while the other 8 subjects needed more trials to correct movement errors. Of these 8, 3 subjects tended to make only inadequate attempts to correct the error.
Discussion and Conclusion
Discussion:
We found that healthy subjects use the same strategies of correction at slower speeds than those observed when moving as fast as possible which confirmed that movement speed was not responsible for the observed differences in correction patterns between healthy and hemiparetic subjects. Less affected subjects corrected movement errors in less than 3 trials as seen for normal subjects whereas those whose sensorimotor deficits were more severe either did not correct movement errors or made slow, inconsistent corrections.
Our results suggest that the ability to use short-term error correction strategies may be related to the level of sensorimotor impairment after a stroke. From our data, we defined three "learning skills" groups corresponding to high, medium and low sensorimotor impairment according to the Arm Function sub-section of the Fugl-Meyer Scale. These groups were characterized by different patterns of error correction for accurate elbow flexion after the sudden application or removal of an external load. Subjects in the first group (Fugl-Meyer score 50-60: mild to no motor deficit) used error correction strategies similar to those in healthy subjects as described in Weeks et al. (1996) and tended to improve in movement precision and speed over the 120 trials. Subjects in this group would be fully capable of improving their motor skills after treatments based on movement repetition. Subjects with moderate motor disability (Fugl-Meyer score 25-40) often needed two, three or even four trials to correct movement errors. However, during the course of repetition, there was an improvement in the number of trials needed for correction and an increase in the movement precision. These subjects would fall into an "intermediate" group of hemiparetic patients who could benefit from movement repetition but, who would require a great deal of time and effort to teach these new tasks. A third group of subjects who were more severely affected (Fugl-Meyer score 10-15) did not use any correction strategy and did not improve their performance even after 120 trials. For these subjects, repetitive movement treatment approaches may not be appropriate.
Acknowledgment: This research was founded by the NSERC and MRC
References
References:
- Feldman, AG (1966) Functional tuning of the nervous system with control of movement or maintenance of a steady posture. Biophysics 11: 667-675.
- Feldman, AG and Levin, MF (1995) Positional frames of reference in motor control. The origin and use. Behav. Brain Sci. 18: 723-806.
- Flanagan, JR , Ostry, DJ, and Feldman, AG (1993) Control of trajectory modifications in target-directed reaching. J. Mot. Behav. 25: 140-152.
- Flash, T and Henis, E (1991) Arm trajectory modifications during reaching toward visual targets. J. Cognit. Neurosci. 3: 220-230.
- Lackner, JR and Dizio, P (1994) Rapid adaptation to Coriolis force perturbations of arm trajectory. J. Neurophysiol. 72: 1-15
- Shadmehr, R and Mussa-Ivaldi, FA (1994) Adaptive representation of dynamics during learning of a motor task. J. Neurosci. 14: 3208-3224.
- Van Sonderen, JF and Denier Van Der Gon, JJ (1990) A stimulation study of a programme generator for centrally programmed fast two-joint arm movements: reponses to single- and double-step displacements. Biol. Cybern. 63: 35-44.
- Weeks, DL, Aubert, M-P, Feldman, AG, Levin, MF (1996) One-trial adaptation of movement to changes in load. J. Neurophysisiol. 75: 60-74.
| Discussion Board | Previous Page | Your Poster Session |