Dermatology Poster Session
| INABIS '98 Home Page | Your Session | Symposia & Poster Sessions | Plenary Sessions | Exhibitors' Foyer | Personal Itinerary | New Search |
Introduction
Pachydermodactyly is a rare non-inflammatory bulbous swelling involving the dorsal and lateral surfaces of the fingers at the level of proxymal phalanges and interphalangeal joints. Histopathologic features include increased dermal accumulation of collagen, sometimes entrapping eccrine glands and occasionally an increased number of fibroblasts. No inflammatory infiltrate is visible. We describe a typical case of pachydermodactyly in a young man.
Case Report
A 22-year-old man presented with a 10-year history of asymptomatic persistent symmetrical swellings on the lateral and medial aspects of fingers II - III bilaterally.No family history of similar diseases, nor history of trauma was recorded. X-rays of the hands showed only soft tissue swellings (Fig.1).
 Click to enlargeFig. 1: Clinical picture.
Click to enlargeFig. 1: Clinical picture.
Histopathologic examination of a biopsy specimen revealed hyperkeratosis, hypergranulosis overlying a markedly thickened dermis, consisting of increased collagen bundles sometimes haphazardly arranged, slight proliferation of blood vessels, increased number of fibroblast and slight perivascular lymphocytic infiltrate (Fig.2, Fig.3). After two years the clinical picture was unaffected.
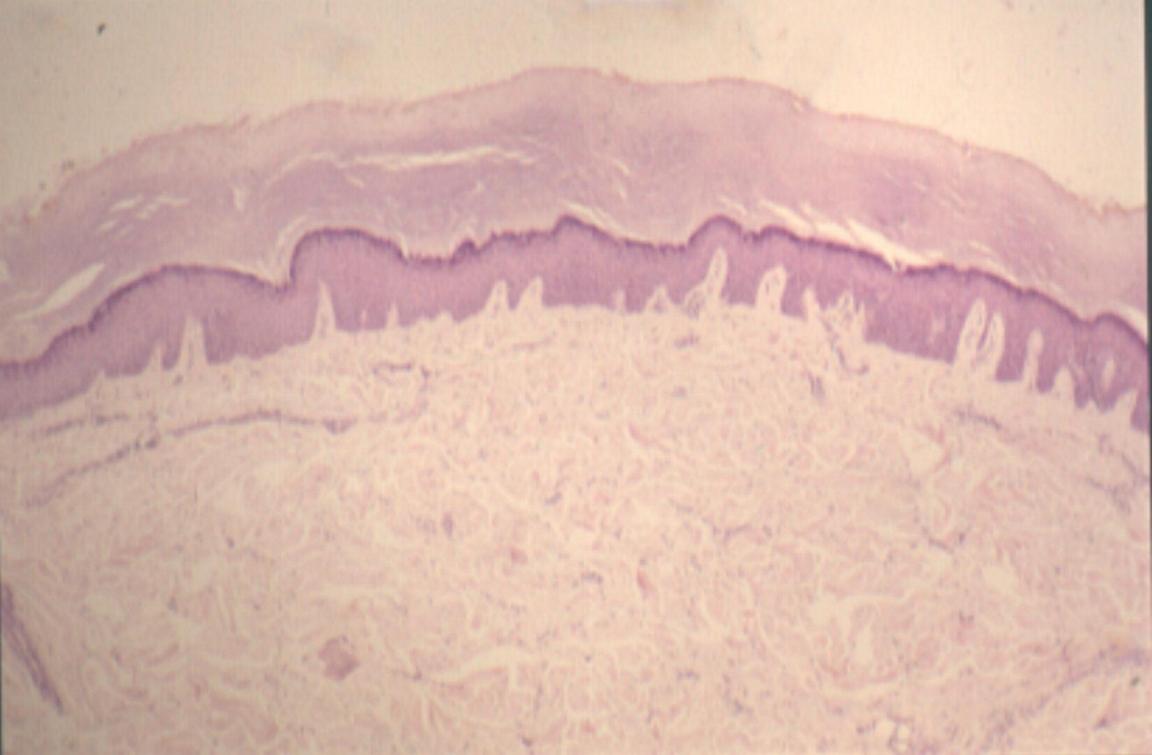 Click to enlargeFig. 2: Haematoxylin-eosin, 4x.
Click to enlargeFig. 2: Haematoxylin-eosin, 4x.
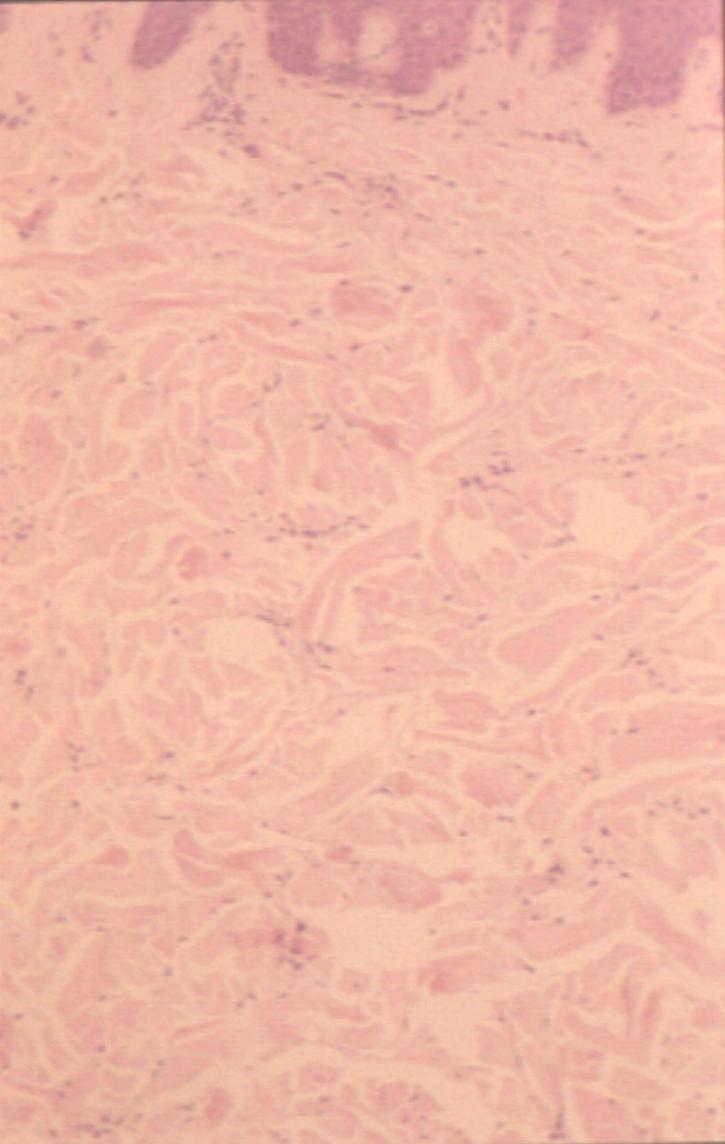 Click to enlargeFig.3: Haematoxylin-eosin, 10x.
Click to enlargeFig.3: Haematoxylin-eosin, 10x.
Discussion
Pachydermodactyly was first described by Bazex el al. in 1973, but it was recognized by Verbov in 1975 as a variant of knuckle pads. It affects almost exclusively young males, but a few females have been reported. Generally the second, third and fourth fingers are affected simmetrically and bilaterally. Only four cases of pachydermodactyly localized to one finger have been reported. Distal fingertips location is a rare variant. It is an acquired disease, with a single report of familial occurence. Associations with tuberous sclerosis, atrophia maculosa varioliformis cutis, carpal tunnel syndrome and gynecomastia have been reported. In the majority of cases aetiology is unknown, but several hypotheses take into account repeated trauma, sometimes in the background of obsessive-compulsive behaviour. The isolation of collagen from the involved sites has revealed large amounts of collagen types I, III, and V, which differ from the collagen profile of normal skin. The nosologic position of pachydermodactyly is not clear yet. Some Authors include this dermatose among fibromatoses, but others do not accept such a view because there is no true proliferation of fibrocytes, nor important inflammatory infiltrate, but merely increased collagen production. Differential diagnosis is mainly made with knuckle pads, post-traumatic callosities, foreign-body granulomas, fibromas, infantile digital fibromatosis, degenerative collagenous plaque of the hands, acrokeratoelastoidosis, rheumatoid and pseudo-rheumatoid nodules, arthritis, thyroid acropachy, pachydermoperiostosis and proteus syndrome. Topical treatment with corticosteroid is ineffective, intralesional steroid injection gives contrasting results. Psycotherapy or surgical excision in selected cases may be an effective option.
References
- Draluck JC, Kopf AW, Hodak E. Pachydermodactyly: first report in a woman. J Am Acad Dermatol 1992;27:303-5.
- Aloi F, Solaroli C, Tomasini C. Pachidermodattilia e cuscinetti delle falangi: dermatosi autoprovocate? G Ital Dermatol Venereol 1993;128:393-7.
- Dupin N, Gautier MS, et al. Pachydermodactylie Ann Dermatol Venereol 1994;121:632-4.
- Paricio JF, Lopez MA, et al. Pachydermodactyly limited to one finger. Eur J Dermatol 1995;5:338-42.
- Kopera D, Soyer HP, Kerl H.. An update on pachydermodactyly and a report of three additional cases. Br J Dermatol 1995;133:433-7.
- Callot V, wechsel J, Hovnanian A, Revuz J. Pachydermodactyly and atrophia maculosa varioliformis cutis. Dermatology 1995;190:56-8.
- Itin PH, Lautenschlager S. Pachydermodactyly: a psychocutaneous disorder. Dermatology 1995;190:1-3.
- Veraldi S, Rizzitelli G, Brusasco A, Giannotti R. Pachydermodactyly of a single finger. Eur J Dermatol 1996;6:576-8.
- Tompkins SD, McNutt NS, Shea CR. Distal pachydermodactyly. J Am Acad Dermatol 1998;38:359-62.
| Discussion Board | Previous Page | Your Poster Session |