Cancer Poster Session
| INABIS '98 Home Page | Your Session | Symposia & Poster Sessions | Plenary Sessions | Exhibitors' Foyer | Personal Itinerary | New Search |
CLINICAL HISTORY
A 47 year-old male that was diagnosed of diffuse large B-cell lymphoma stage IVA, with intestinal, splenic and retroperitoneal lymph nodes affectation, one year ago. After 6 chemotherapy cycles (CHOP), the splenic mass measuring 13 cm in diameter and peri-splenic adenomegalies persisted. Splenic radiotherapy was performed and three new cycles of the same scheme were administered. In the following reappraisal, they still persisted, and 6 chemotherapy cycles of FMD (fludarabine, mitoxantrone and dexametasone) was administered with acceptable hematological and clinical tolerance. Thereafter, a CT scan showed the persistence of the splenic mass and the peri-splenic adenomegalies (figure1).
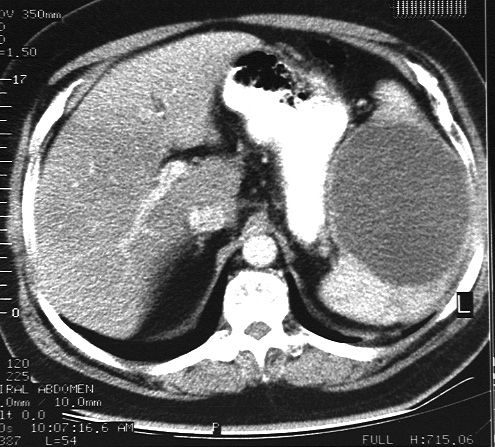 Fig.1: CT-scan.
Fig.1: CT-scan.
No others anomalies were detected in a complete revision. The possible diagnoses were persistence of the lymphoproliferative process, and a splenic infarct. A splenectomy and peri-splenic lymphadenectomy were performed with diagnostic and therapeutic aim.
MATERIAL AND METHODS
The spleen and lymph nodes were routinely fixed in buffered formalin, sectioned at 5 m, and stained with hematoxylin and eosin for morphologic studies. For immunohistochemistry, deparaffinized, rehydrated sections were treated with 3% H2O2 in methanol for 30 minutes at room temperature to abolish endogenous peroxidase activity. Tissue sections were treated with trypsin (Sigma Chemical Co., St Louis, MO) for 10 minutes at 37şC and microwaves. After overnight incubation at 4şC with the primary antibody, slides were washed in phosphate-buffered saline (PBS) and then exposed to the biotinylated secondary antibody dilutes at 1:100 in PBS, for 1 hour at room temperature. They were then washed in PBS for 10 minutes and incubated for 60 minutes with the streptavidin-biotin-peroxidase complex (1/100; Biogenex) at room temperature. Using these techniques sections were reacted with antibodies against CLA (CD45, Biogenex), UCHL-1 (CD45RO, Biogenex), CD20 (Dako), CD43 (Biogenex), CD3 (Zymed), and keratins (Biogenex). The slides were counterstained with Harris’s hematoxylin, dehydrated, cleared and mounted.
PATHOLOGIC FINDINGS
The spleen measured 19 x 13 x 6 cm and it weighed 850 g. It was deformed for a mass that measured 13 cm of diameter. The lesion was well circumscribed and relatively homogeneous. The cut surface had a yellow color and a necrotic aspect (figure2). Peri-splenic lymph nodes showed a similar gross appearance.
 Fig.2: Gross feature of the cut surface of the spleen.
Fig.2: Gross feature of the cut surface of the spleen.
Histologic examination of the splenic mass and peri-splenic lymph nodes showed massive coagulative necrosis, a confluent sheet of eosinophilic necrotic material with areas showing the silhouettes of necrotic cells (figure3). No inflammatory cell infiltrates and nuclear karyorrhexis were seen. Necrotic cells were also found within normal splenic parenchyma (figure 4).
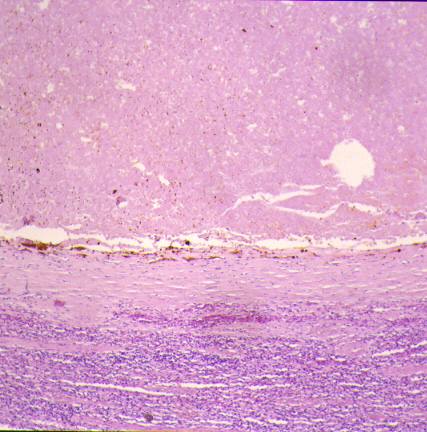 Fig.3: H/E x100.
Fig.3: H/E x100.
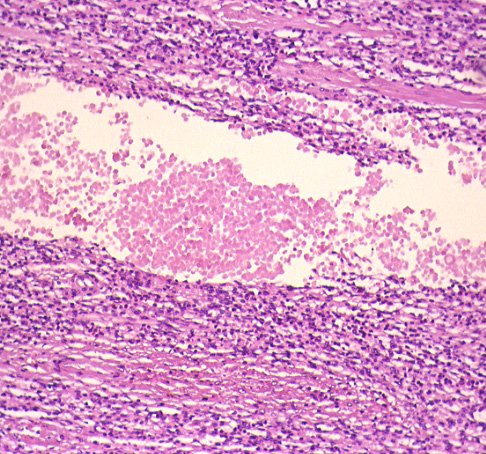 Fig.4H/E x 200.
Fig.4H/E x 200.
The most necrotic cells had a strong surface membrane reactivity with CD45 (CLA), and CD20 (L26) (Fig.5-6).
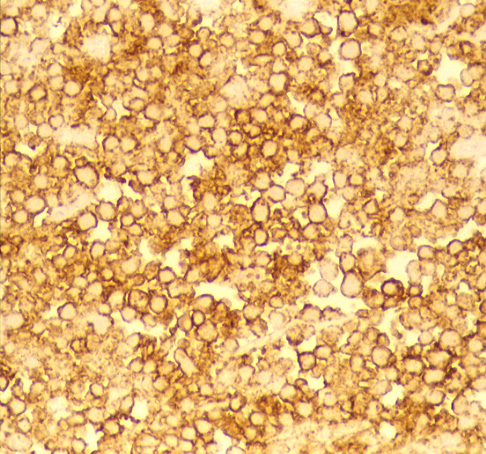 Fig.5: CD20 (immunoperoxidase x 400).
Fig.5: CD20 (immunoperoxidase x 400).
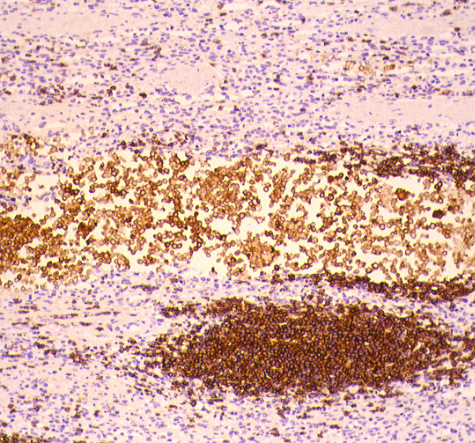 Fig.6: CD20 (immunoperoxidase x 200).
Fig.6: CD20 (immunoperoxidase x 200).
CD3, CD43 (MT1), CD45RO (UCHTL-1) and keratins were uniformly negative in the necrotic cells (figure 7).
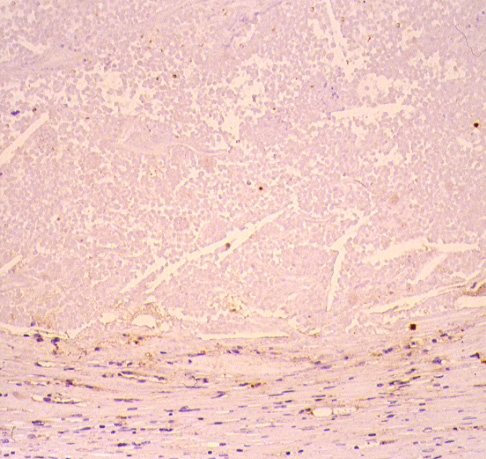 Fig.7: CD3 (immunoperoxidase x 200).
Fig.7: CD3 (immunoperoxidase x 200).
No background staining was present in the necrotic tissue with any of these antibodies. This immunophenotypic data suggested a diagnosis of necrotic B cell lymphoma.
DISCUSSION
Residual masses may occur following irradiation and/or chemotherapy for Hodgkin’s disease 1 and germ cells tumors2, but it is uncommon in non-Hodgkin’s lymphomas3-5. The finding of these residual masses raises problems of approach. The appropriate filiation of these masses can change our attitude drastically with the patient's handling; complete response versus partial or no response than requires an intensified chemotherapy. Nowadays, surgical histology reevaluation is the most reliable method of evaluation the viability of tumor residual masses 4. Recently, it has been postulated that positron emision tomography (PET) may offer the possibility of differentiating vital from necrotic residual masses6. Also, biochemical markers such as an elevation of the serum LDH could be useful to suggest viable lymphoma7, nonetheless, a normal value certainly does no exclude it8. At present, until new radiological or biochemical markers are available, a judicious clinical attitude should be taken, with radiological control of the evolution of the masses and reserving surgery for those cases with diagnostic doubts.
In general, tumors composed of a single or multiple large nodules in the spleen, usually result from involvement by diffuse large cell lymphoma, follicular large cell lymphoma, Hodgkin’s disease, malignant fibrous histiocytoma, metastasis, and inflamatory pseudotumor. The miliary pattern or small white nodules involving the entire parenchyma, is seen predominantly in small cell lymphomas, follicular lymphomas, B-cell chronic lymphocytic leukemia, miliary tubeculosis, and amyloidosis.
Preservation of antigenicity in lymphoid cells showing the histological features of coagulative necrosis was demonstrated by Pallesen and Knudsen9. Norton et al, in their study have reported the contribution of immunostaining using monoclonal antibodies to fixation-resistant leucocyte antigens in making the diagnosis of lymphoma, in the presence of coagulative necrosis of the entire lymph node10. The surface membrane pattern of binding of these antigens provided an easy method for assessing the specificity of immunohistology in the necrotic cells10,12. Coagulative necrosis implies preservation of the basic outline of the cell, presumably the increasing intracellular acidosis denatures not only structural proteins but also lysosomal enzymes and so blocks the proteolysis of the cell.
We have checked that the immunostaining with a panel of reagents to fixation-resistant leukocyte antigens and antibodies to non-leucocyte antigens provide valuable complementary information to conventional histology in the assessment of coagulative necrotic tissues11. A series of known tumors consisting of 5 carcinomas, 4 sarcomas, 2 melanomas, 2 lymphomas and 1 pituitary adenoma (all with extensive necrosis but with viable cells) was examined for reactivity with: cytokeratin antibodies (AE3/AE1, CAM 5.2 and PANCK), EMA, Vimentin, O13, S100, HMB45, estrogens, progesterone, antibodies to leucocyte antigens, immunoglobulins and chromogranin.
The antibodies that showed the most consistent reactivity in necrotic tissue were LCA (CD45), UCHL-1 (CD45RO), MB2, EMA, AE3/AE1, CEA, PANCK, CAM5.2, chromogranin, and O13 (CD99). Only patchy peripheral immunorreactivity with L26 (CD20), S100 and HMB45 was seen in necrotic tissue. Estrogens, progesterone, immunoglobulins, and vimentin were of little or no value in the necrotic material. No background staining was present in the necrotic tissue with any of these antibodies11.
In this case, the unexpected histological diagnosis made us consider the patient in remission against the initial hypothesis of residual viable mass. At present (8 months later), the patient does not receive treatment, staying in clinical remission.
REFERENCES
- Jockelson M, Mauch P, Balikian J, Rosenthal D, Canellos GP (1985) The significance of the residual mediastinal mass in treated Hodgkin’s disease. J Clin Oncol 3:637-640.
- Vogelznag NJ, Stenlung R (1983) Residual pulmonary nodules after combination chemotherapy of testicular cancer. Radiology 146:195-197.
- Montalban C, Arechaga S, Calleja JL, Bellas C, Patier JL, Berenguer A et al (1990) Intraparenchymal non-neoplastic residual masses after treatment of large-cell non-Hodgkin’s lymphoma with intensive chemotherapy. Med Clin 94:461-464.
- Mandelli F, Amadori S, Guglielmi C, Martelli M, Coluzzi S (1991) Clinical and pathological restaging in aggressive non-Hodgkin’s lymphomas. Leukemia 5 (Suppl 1):38-41.
- Surbone A, Longo DL, de Vita VT, Ihde DC, Duffey PL, Jaffe ES, et al (1988) Residual abdominal masses in aggressive non-Hodgkin’s lymphoma after combination chemotherapy: significance and management. J Clin Oncol 6:1832-1837.
- De Wit M, Bumann D, Beyer W, Herbst K, Clausen M, Hossfeld DK (1997). Whole-body positron emission tomography (PET) for diagnosis of residual mass in patients with lymphoma. Ann Oncol 8 (Suppl 1):57-60.
- Ballas M, Sanchez M, Lee JH, Czepiel SJ, Kashani M (1982). Syndrome of the infarcted lymp node. Lab Invest 46:7.
- Cleary K, Osborne BM, Buler JJ (1982). Lymph node infarction forshadowing malignant lymphoma. Am J Surg Pathol 6:435-442.
- Pallesen G, Knudsen LM (1985). Leucocyte antigens in post mortem tissues: their preservation and loss as demonstrated by monoclonal antibody immnohistological staining. Histopathology 9:791-804.
- Norton AJ, Ramsay AL, Isaacson PG (1988). Antigen preservation in infarted lymphoid tissue. Am J Surg Pathol 12:759-767.
- Vega F, Lozano MD, Okafor OC, Fernandez J, Pardo-Mindán FJ (1998). Utility of immunophenotypic studies in necrotic tissues [Abstract]. Paper presented at the 87th Annual Meeting of the United States and Canadian Academy of Pathology, Boston :188.
- Vega F, Lozano M.D., Alcalde J, Pardo-Mindán F.J (1998). Role of the inmunohistochemical and Molecular Biology in necrotic lymph node. Virchows Archives. (In Press.
| Discussion Board | Previous Page | Your Poster Session |