Poster
Content
| INABIS '98 Home Page | Your Poster Session | Related Symposia & Posters | Scientific Program | Exhibitors' Foyer | Personal Itinerary | New Search |
John D. Denstedt, M.D. (Department of Urology, University of Western Ontario, Canada)
Gregor Reid, Ph.D (Department of Immunology and Microbiology, University of Western Ontario, Canada)
Current Situation
In recent years, there have been many attempts to harness computer and internet technologies for professional education and patient management across a broad spectrum of medical disciplines including endocrinology (1,2,3,4), radiology (5,6,7), surgery (8,9,10), family medicine (11,12,13,14) oncology (15,16) and asthma (17,18,19), among others.
In addition, many academic institutions have endeavored to develop internet-based learning programs in medicine. The table below summarizes several such efforts:
In addition to these efforts, the global urology community is represented by a number of credible web pages recommended for their design, navigation and content. These include the American Urological Association, the Endourological Society, the National Bladder Foundation, the European Association of Urology and the Digital Urology Journal.
Clearly, there are many other urolgy web sites, but those cited here represent good places to begin exploring urology-related information found on the Internet. Content within these and other urology-related sites is generally developed for a wide variety of professional and consumer audiences and, while successfully serving the communication needs of these organizations, are not focused on structured and continued learning for medical professionals.
Current Challenges
These and other projects have led many to conclude that the internet will become the vehicle for ongoing learning and exchange of ideas in medicine. Internet based resources for physicians must be continually available and demand the highest possible level of quality control (26). Further, the internet is an effective method of providing CME (27) and physicians and health care providers are strongly motivated to engage in ongoing computer and online-based education (28).
Despite this genuine enthusiasm, we believe there are a number of emerging logistical and practical challenges facing developers and administrators of digital and hybrid media-based programs. These challenges can be characterized as people, technology, content, and learning principles. It is our view that these four components are requisite for successful learning program development, launch and ongoing refinement (29).
People: Successful program development and ongoing refinement require the pooled talents of a number of disciplines. These include designers of digital media, designers of conventional media, skilled programmers across a variety of platforms, data base server and web server support personnel, corporate identity and message strategists, content experts and "knowledge engineers". This diverse group of highly trained individuals must be free to dedicate the necessary time and resource for successful program development, launch and ongoing refinement. These requirements may often exceed available resources of many academic institutions.
Technology: The challenge posed by digital technology is several-fold. It involves keeping abreast of current and future developments, the scalability to encompass multiple mediums into program development, the ability to reach "critical mass" and complete and maintain programs once a prototype is developed, data base and web hosting server capability, and hardware system design, installation, maintenance and upgrades. In many cases, these challenges may go beyond the available resources of many academic institutions.
Content: To gain acceptance by learners, content must possess a number of attributes. Content in any learning program must be credible, comprehensive and impartial. Clearly, those content experts who develop learning programs in medicine understand these requisites and have little difficulty fulfilling their requirements. Yet, when a search of the term 'urology' using a standard Internet search engine can yield up to 175,000 web pages, learners are faced with the overwhelming task of evaluating which of these sources of information and knowledge are credible, comprehensive and impartial.
In addition to these requisites, however, we believe content must be timely and of enduring value to learners. Content which is not continually developed and refined will soon lose the ongoing interest of learners.
Further, our position is that learning programs developed by globally recognized experts in a given medical field should be made accessible to global audiences of learners. This has important implications for how best to disseminate content to global audiences which cover the broadest possible spectrum with respect to access to digital technology.
Learning Principles: The final challenge that faces developers of learning programs is how best to structure and present content in a manner that follows sound principles of learning and distance education. Such structure and presentation of content requires extensive knowledge of both curriculum design and functionalities of current and future digital technology. By bringing together these two knowledge sets, we believe optimal program design enables self-directed, user-centered learning which addresses clear, measurable objectives through prudent application of media technology. We have established a number of so-called "Learning Stations" which, in our view, represent the optimal harmonization of curriculum design, learning strategies, and digital technology.
Given these four challenges, the Lawson Research Institute realizes that, while it is comprised of world-recognized experts who have created a knowledge base which is credible, comprehensive, impartial and of global interest, it does not have the resources necessary to successfully disseminate this knowledge base. It further understands that these resources are found within the private sector. This has led to the partnership involving the Lawson Research Institute and Axia NetMedia Corporation to collaboratively develop the programs described in the remainder of this poster.
Program Objective
The Urology Learning Program (ULP) is being developed to assist the Lawson Research Institute realize its mandate of returning to its funding public the meaningful and practical results of its ongoing research and clinical practice. This cumulative knowledge base, the result of the ongoing work and contributions of approximately 100 primary researchers and clinicians, is serving as the basis upon which the hybrid media ULP is being developed.
The ULP is comprised of a number of content modules, each with its own target audience, set of learning objectives and learning strategies. To date, two such modules have been created: Urinary Tract Infection in Women (Figure 1) and Ureteroscopy for Urologists (Figure 2). Other topics, including erectile dysfunction, prostate disorders, bladder cancer and incontinence, are currently being developed.
Once developed, health care practitioners will have three ways to access the ULP: CD-ROM, Internet and conventional media. The Ureteroscopy for Urologists Module will be available to urologists world-wide in 1999.
Program Description
Each module of the ULP consists of three integrated components: CD-ROM, Internet and conventional media. Each of these components is described below.
The CD-ROM contains high bandwidth reference material including video, animations, images and audio. We regard current CD-ROM technology as a suitable vehicle for transfer of high bandwidth content until the balance of the target audience for this program has unrestricted high bandwidth internet access.
Given that updating and distributing CD-ROM-based content presents unique challenges, we regard this component of the ULP as housing reference material generally accepted within the global medical community as constituting sound and effective urologic understanding and management. The content of the ULP CD-ROM will be updated on an annual basis to reflect ongoing accumulation of new content within the Internet portion of the program. In this way, the reference content of the ULP will remain current.
Several student-centric, self-directed learning strategies are being applied to the ULP reference material. The Overview presents a summary of the fundamental principles of topic centric epidemiology, pathophysiology, treatment and ongoing management (Figure 3). This information is presented through digital video, audio, animation, images and text.
Other student-centric, self-directed learning strategies being applied to the ULP content include "Comparative Learning", wherein disparate or very similar concepts can be compared across a number of characteristics (Figure 4). In this example, the learner is free to explore diagnostic challenges of urinary tract infection, such as anatomy, pathophysiology, history and symptoms and signs, through comparision of these arttibutes across both bladder and kidney forms of infection. Video, audio, animations, images and text are used to crystallize these comparisons.
The "Skill Sequencer" parses or breaks down complicated skills into their fundamental steps for study and review (Figure 5). Learners come to understand a complicated skill in its entirety through self-directed study and review of its component or fundamental parts. In this example, video is used to break down the skill of ureteroscopy into its fundamental steps. This skill is challenging to first time learners who will be charged with the task of competently performing this intervention on patients.
In "Challenge Mode", learners freely explore their understanding of content through self directed questions and answers. A question is posed based on the media and accompanying list of possible answers shown on the left side of the screen. If the correct answer is chosen, the learner receives positive feedback. For an incorrect answer, the question on the screen is replaced by examples of media reflecting that incorrect answer. In this way, the learner is able to simultaneously compare media describing both correct and incorrect answers (Figure 6).
The Internet component of the ULP enables the global urology community to gather and engage in ongoing discussion, exchange information and participate in accredited educational activities. We describe this ongoing discussion, accredited educational activity and posting of new knowledge as "Dynamic Publishing".
This Dynamic Publishing model is the digital equivalent of conventional media publishing. That is, new content is posted following a predetermined publishing schedule, in which dates for presentation and discussion of specific topics, such as urolithiasis or post-operative complications, are established.
This schedule of dynamic publishing is made known to participants thereby enabling them to establish their own schedule for visiting and spending time at the web site. In this way, participants are encouraged to return to the ULP Internet Site on a recurring basis to engage in ongoing learning of topics of individual interest and relevance.
The functionality necessary for Dynamic Publishing is, in our view, threefold. The Forum, enables both real-time and ongoing discussion of predetermined urology topics. These discussions are regarded as 'events' wherein urology experts are accessible to the global urology community to share their expertise and experience (Figure 7).
In the Reading Room, urology experts and others will post new content in the form of preliminary research results, completed research, papers and related news and information, again following the predetermined schedule of urology topics (Figure 8).
Finally, the Testing Centre enables participants to engage in accredited educational activities. As the Testing Centre also follows the schedule of topics for a given module within the ULP web site, learners are able to take advantage of both the Forum and the Reading Room prior to undertaking these accredited educational activities (Figure 9).
The Conventional Media component of the ULP enables those without computer hardware or access to bandwidth to participate in this program. Conventional media is integrated into the entire GLP through careful attention to both design and structure of content such that learners can make the seamless transition to the digital side of the ULP once they gain access to digital technology (Figure 10).
The primary format of conventional media is print but will also include, as need dictates, video tape, audio tape, television and radio. These strategies are necessary in the sense that programs with a mandate for global accessibility must accommodate those without access to digital technology. Current estimates of global access to the Internet range from 12 to 16 per 1000 population (30).
Summary
Digital technology is being harnessed to develop educational programs across a broad spectrum of medical disciplines. Typically, these programs have been developed for small, localized audiences and are integrated into more complete and conventionally delivered medical curricula. In addition, many national and international urology organizations have developed very comprehensive and well designed web sites. Content within these sites is generally developed for a wide variety of professional and consumer audiences and, while successfully serving the communication needs of these organizations, are not focused on structured, ongoing and formal learning for professionals. Professionals are also faced with the challenge of sifting through an overwhelming number of web sites and programs devoted to urology and must contend with issues of timeliness, comprehensiveness, credibility and impartiality.
We have described the current development of a global learning program based upon content developed by the Lawson Research Institute. This Urology Learning Program (ULP) is being developed to assist the Lawson Research Institute realize its mandate of returning to its funding public the meaningful and practical results of its ongoing research and clinical practice. Through integration of CD-ROM, Internet and conventional media strategies, the ULP is described as a hybrid media program wherein Dynamic Publishing takes places. Further, the ULP addresses the issues of timeliness, comprehensiveness, credibility and impartiality by being based upon the collaborative effort involving approximately one hundred principle investigators of the Lawson Research Institute. The Ureteroscopy of Urologists module of the ULP will be distributed world wide beginning September 1999.
References
Topic Developer/Provider Computers in Medicine Boston University Biology of Cancer Syracuse University Histology National University of Singapore Physiology University of Arizona Anatomy University of Washington
In urology, digitally-based learning programs have been developed for not-for-profit urology groups (20), on-line chat and information sharing (21), general urology information (22), medical student education (23), data storage of urologic images (24), and development of urologic multimedia presentations (25). Generally speaking, these programs are developed for relatively small, localized audiences and are integrated within more complete and conventionally delivered medical curricula.
 Figure 1. UTI in Women Opening Screen
Figure 1. UTI in Women Opening Screen
(click image to enlarge)
 Figure 2. Ureteroscopy for Urologists Opening Screen
Figure 2. Ureteroscopy for Urologists Opening Screen
(click image to enlarge)
 Figure 3. UTI in Women Overview
Figure 3. UTI in Women Overview
(click image to enlarge)
 Figure 4. UTI in Women Comparative Learning
Figure 4. UTI in Women Comparative Learning
(click image to enlarge)
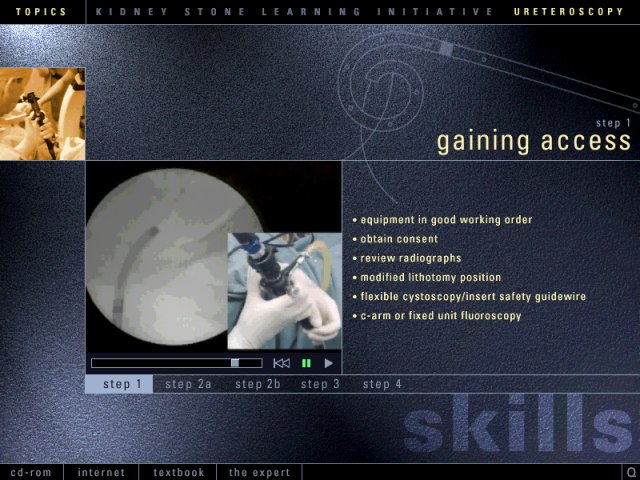 Figure 5. Ureteroscopy for Urologists Skill Sequencer
Figure 5. Ureteroscopy for Urologists Skill Sequencer
(click image to enlarge)
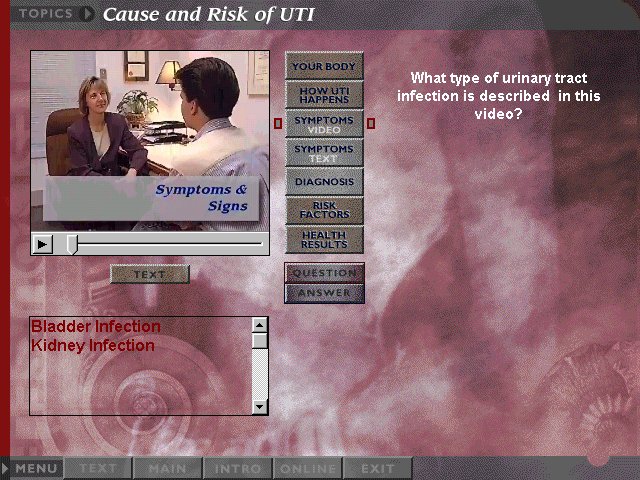 Figure 6. UTI in Women Challenge Mode
Figure 6. UTI in Women Challenge Mode
(click image to enlarge)
 Figure 7. Ureteroscopy for Urologists Internet Forum
Figure 7. Ureteroscopy for Urologists Internet Forum
(click image to enlarge)
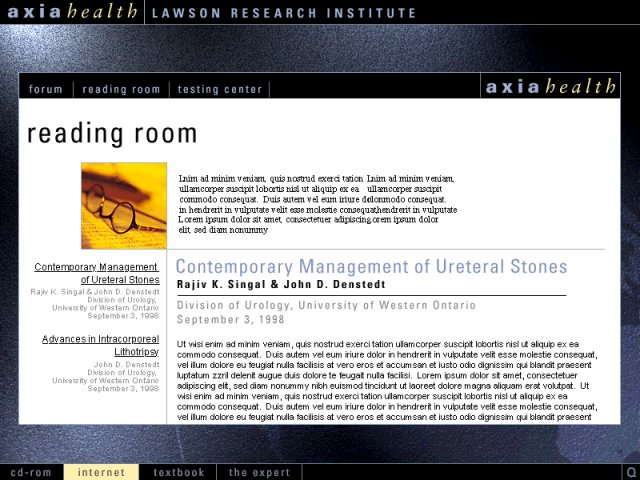 Figure 8. Ureteroscopy for Urologists Internet Reading Room
Figure 8. Ureteroscopy for Urologists Internet Reading Room
(click image to enlarge)
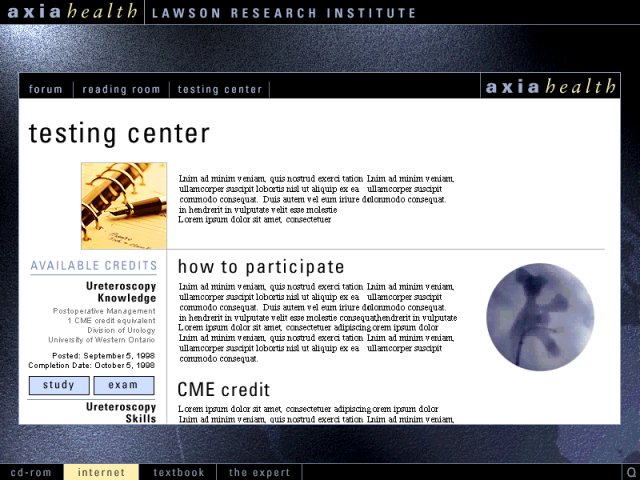 Figure 9. Uteroscopy for Urologists Internet Testing Centre
Figure 9. Uteroscopy for Urologists Internet Testing Centre
(click image to enlarge)
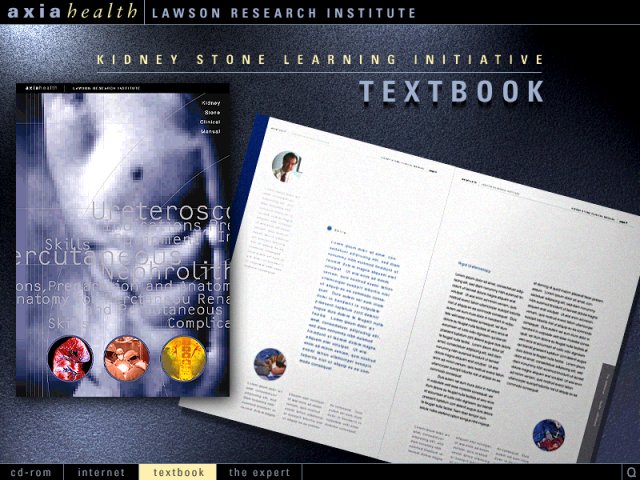 Figure 10. Ureteroscopy for Urologists Conventional (Print) Media
Figure 10. Ureteroscopy for Urologists Conventional (Print) Media
(click image to enlarge)
Back to the top.
Presentation Number PAjohn h. parker0268
Keywords: multimedia,education,urology,ureteroscopy,UTI
| Discussion Board | Previous Page | Your Poster Session |