The patient is a 57 year old right handed male self
employed drywaller. Date of birth 7 May 1941. Age 49 at the time of the index injury, an
innocuous looking distal radius fracture after fall on the
outstretched hand (Injury 2 Dec 1990).
This was treated by the Emergency Room Physician with a forearm cast. He was followed by
his general practicioner.
By Feb 25th 1991 the fracture was not healing, had shortened
and angulated.He was referred to an orthopaedic surgeon.
Internal Fixation and bone grafting was done on 27th Feb 1991.
Xray taken 7th March 1991 shows the fracture aligned, bone
grafted and fixed with a T plate. The bone was sufficiently abnormal for the surgeon to
take a specimen for pathological examination. This specimen is no longer available but the
report indicated a "chronic inflammatory infiltrate".
By 13th June 1991 it was noted that the fixation was not
holding and the fracture began to displace.
Xray of 28th October 1991 showed significant loss of bone at
the non-union site. The bone graft is reabsorbed or fragmenting and there is now
significant osteopaenia in the surrounding bone, notably the ulna and the carpal bones.
Wrist Fusion from the
Long finger metacarpal to the radius with resection of ulnar head was undertaken Jan 1992
However, further views taken 10th July 1992 showed reabsorption
of bone from the distal ulna and no healing of the fusion. (R)
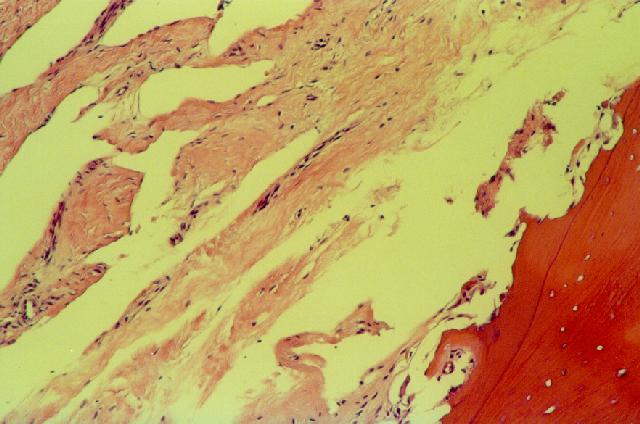
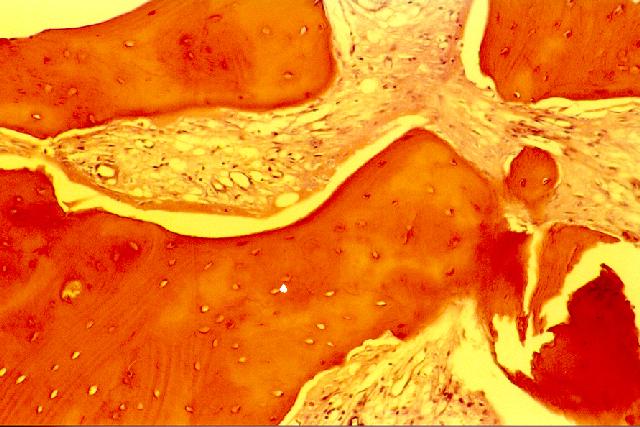
Biopsy of distal L ulna 1993.Ectatic vessels
are seen involving the periosteum and adjacent soft tissue. Consistent with but not
pathognomonic of the diagnosis of Gorham's Disease.
He was managed non-operatively for 3 years during which time he did return to work as a
dry-waller using his right hand only.
In 1994 he was referred to a tertiary centre for consideration of vascularized
fibular graft. A further biopsy was undertaken and the diagnosis of Gorham/Stout
Disease (Disappearing Bone Disease) was made.
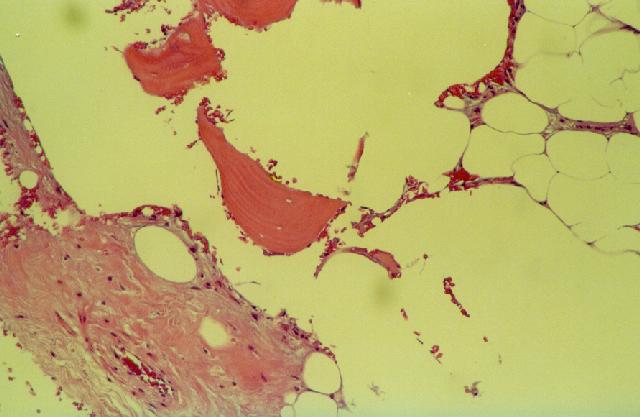
Biopsy L forearm 1994 Cortical and cancellous
bone showing osteoporosis with an increased number of capillaries and small arterioles.
Consistent with Gorham's Disease.
Free vascularized fibular grafting was undertaken bridging from the
proximal ulna to the index finger metacarpal. These Xrays from March
27th 1995 show the extent of the bone loss of the radius and carpal bones
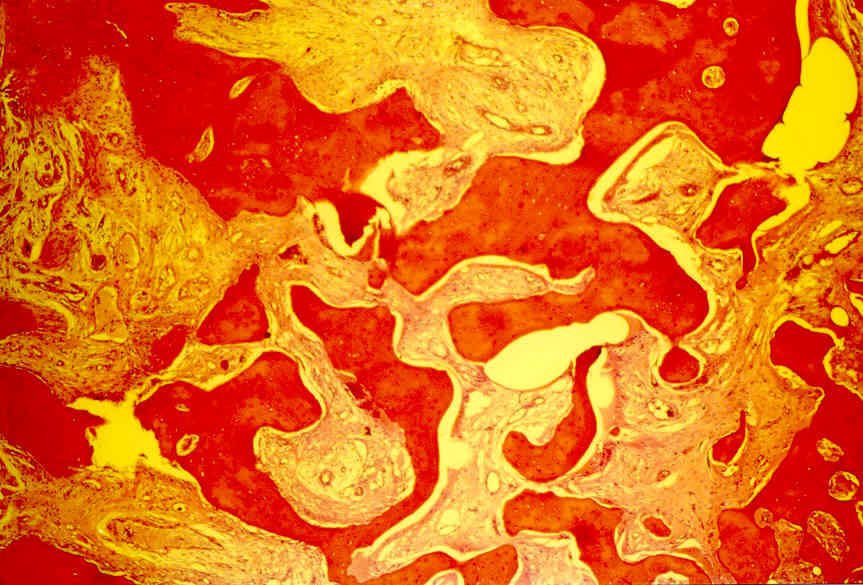
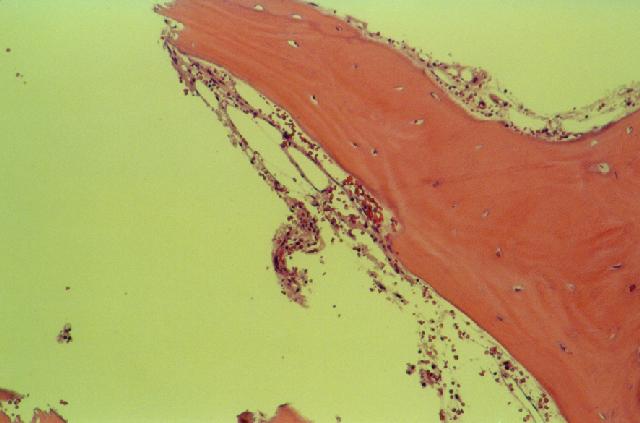
Biopsy L Ulna 1995 Thick and irregularly shaped
trabeculae of bone showing focal areas of necrosis and marrow fibrosis. (detail)
Two further procedures were undertaken, application of a second
plate to the proximal site between the ulna and the fibular graft and radiotherapy.
The patient, at least, attributes the eventual healing of the injury to radiotherapy. He
returned to work once again.
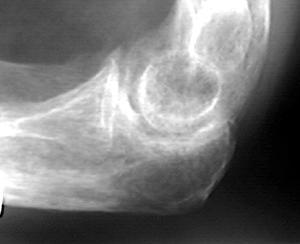
Of note is an xray of the elbow taken in 1995, showing that the olecranon was radiolucent
but intact.(Lateral L elbow 16th Oct 1995).
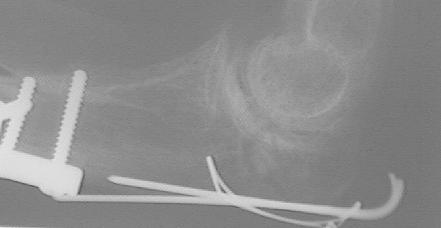
On June 1st 1998 he fell at work
and sustained a Fracture of Left (ipsilateral) Olecranon
Process. Immediate treatment consisted of open reduction and internal fixation of the
olecranon fracture using standard tension band wiring technique. A bone
biopsy was taken at the same time and showed features typical of Gorham's Disease.
Ancillary treatment consisting of electrical stimulation of the fracture site (Matrix 500 202) and pamidronate 201 infusion (60mg over 4 hours once
weekly for 6 weeks) was begun once the diagnosis was confirmed.
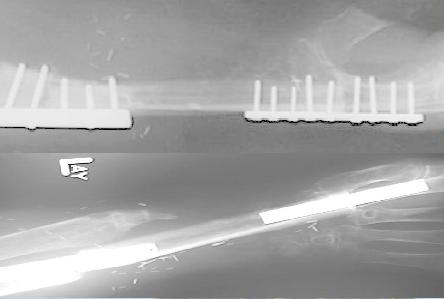
Xray of L Olecranon 9 June 1998, 8 days post ORIF show the
fracture is reduced, compressed and only just visible.
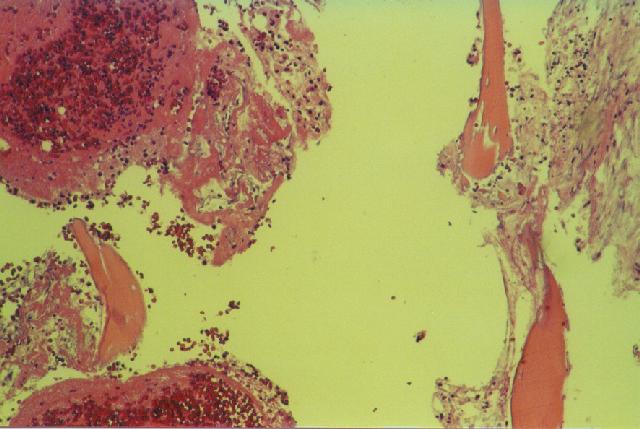
Biopsy from L Olecranon Fracture
June 1998 Haemorrhage and blood clot consistent with recent fracture. Background fibrillary marrow fibrosis and vascular ectasia in keeping with
Gorham's disease.
July 22nd 1998 Radiolucency at the fracture line raises the
possibility of activation of Gorham's Disease at the injury site
August 18th 1998 suggestion of bone
filling in the fracture line may be due to differences in technique. The patient has
returned to work against advice. Radiotherapy was initiated.
September 15th 1988 further evidence of callus. Note on this
view the radiolucencies that have developed around the proximal screws of the old plate on
the ulna. These lucencies have been noted from the June 1st 1998 xray.
Follow-up to November 1998, 5 months post injury continues to indicate the fracture has
healed.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}