| INABIS '98 Home Page | Your Symposium | Related Symposia & Posters | Scientific Program | Exhibitors' Foyer | Personal Itinerary | New Search |
A BALANCED TREATMENT MODEL
A DYNAMIC BALANCED TREATMENT MODEL
D. Geroukalis and A. Panayotopoulos
You can’t discover the bounds of the soul no matter how much you travel towards any direction, this is the depth of its speech.
Heraclitus, 45
INTRODUCTION
These words of Heraclitus indicate the enormous problems of diagnosis and therapy of psychiatric diseases. Substantially, they are a different expression of the famous law: “Not everything is possible”.
The particular characteristics of the psychiatric diseases, where the speech is basic object and basic tool of their examination, does not allow frequently the application of the known processes which are efficient in other medical specialties.
In this era of the Teleinformatics and the psychopharmacology, the existence of a balanced plan for the therapies of the psychiatric diseases, allows the solution of basic problems which have been perplexing psychiatrists for years, not only on the medical level (therapy – resolved) but also on the organizational level (operations – cost).
The nature of psychiatric diseases does not allow, for all the cases, the existence of numerical scales, in a way that the creation of a Balanced Scorecard (BSC) [1] will be possible and largely acceptable.
The known systems Minnesota [2], EPQ [3], boundaries in the mind [4], which helps beneficially the psychiatric diagnosis cannot be taken us scorecards which will guide to a BSC.
Nevertheless, the concept to BSC can be applied since its vision and strategy maybe thought of us representing the therapeutic program of psychiatric diseases. This program must achieve the coordination of all necessary attempts towards a successful outcome. Therefore, the following approach will be based more on the meaning of balance.
The achievement of balance, which is essence the ultimate goal of the Psychiatry, is imposed by the need of the patient’s therapy which is called/will be called to leave in the family and social environment.
General Introduction
The system as a dynamic or constantly changing system of multiple, interacting elements is so deviously characterized by periods of satbility alternating with periods of disorder.
In the language of complexity theory we wuold characterize the system as a particular type of complex system: it is an irreversible, dissipative, non linear self organizing system.
A person anticipates events by constructing their implications, since events nenver repeat themselves, else they would lose their, identity, one can look forward to them only by devising some construction which permits him to perceive two of them in a similar manner.
Symptoms emerge from incompleted cycles of experience, where the patient/client has become unable to fully engage in the cyclical flow.
Communication is made possible only as a self – referential process. This means that communication takes place whithin the social system and not between the social system and environment.
2. THE PERSPECTIVES
The whole philosophy of the therapeutical program is summarized on what the psychiatrist must overcome, but the kind the wide of the psychotherapy or the psychopharmacotherapy is its base.
In the clinics the medical/paramedical stuff is not to act always beneficially on the very variable psychiatric world, without the existence of a specific active plan. This stuff must have embrace and act according to the strategy of therapeutical program.
The requirements of laboratory examinations and for aims fulfill the program which must have security and efficiently control.
Generally, the therapeutical program includes the therapeutical system which will be applied, the self-organization in the psychotherapy and its social contents.
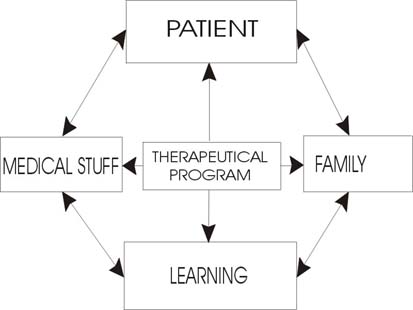
The patient the medical/paramedical stuff and the family of the patient are in intercorrelation and interdependency in the therapeutical program. Learning also must be included in this plan.
In this way the psychiatrist have to act with balance according to four perspectives: Patient, medical stuff, family, learning.
The final goal is of course “to improve the functional status of the patient”. In order to succeed in this goal he follows the Schema 1.
|
The suggested Balanced Treatment Model (BTM) is a referenced in the Psychiatric clinics, where all the four perspectives appear.
Patient
When the psychiatrist meets for first time the patient, he doesn’t know how much time the therapy will last and what will be its results, and especially if he will be the therapeutical doctor until the end.
The psychiatrist generally “annoy”. The more his questions. How should he approach the patient, in order to succeed the best? How does the patient see his doctor? Does he consider him as remarkable and trustworthy? Is it possible to clear the therapeutical goals? How do the control parameters which affects and form the therapeutical program of the patient is chosen?
The patient is not exclusively responsible for his life style. His clinical image, his bio-psycho-social life style, his feeling, his behavior, his work and his environment are the basic elements for the development of the therapeutical program. A clumsy or an inconvenient of the patient expression, is enough to reverse whole scenarios of the psychiatric therapy.
Medical Stuff
The psychiatrist must plan the therapeutical program with some goals, which will discuss with his partners and he will announce it to the paramedical stuff. The disagreements generally in the medical stuff must not create “Babel Tower” circumstances. Also omissions and misunderstandings of the paramedical stuff must not exist. All these conditions affect negative the patient.
Family
The psychiatrist must try to create beneficial conditions for the patient in his family. How should the doctor behave? How does the family see the doctor? Is there a “naďve” ambition or a destructive collapse? Is a family therapy necessary? How a correct explanation of the condition of the patient and for the specific measures which will be taken, will be made? Which roles must be emphasized or disappear?
Usually each one acts alone, without the existence of coordinated process for the patient’s benefit. The confusions which appear, can prove to be destructive.
At the most cases the family web loses its connectivity, when its members have not been informed and trained appropriately. Everybody is involved. Everybody thinks that he “knows” and they play doctor’s role…
For the avoiding of immobilization and corruption of the patient’s family, the members of the family must be trained for the best encounter of his condition.
The adjustment, the cohesion, the communication and the tolerance are the basic elements of the family dynamic in these cases. The interactions must intend to beneficial results.
Learning
Given that the goals of the therapy at most of the times change, the learning of the psychiatrist in new therapeutical methods with wide implications is necessary.
The psychiatric today is a quickly variable space in theories and methodologies. Moreover, the continuously training is needed in order for the psychiatrists to specify and innovate their strategy.
The new psychopharmacology and their proven value, decrease the danger which can caused by misleading indications.
The need for improvement and for better results presume continues learning and access to modern tools of Informatics, such as Healthcare Information Systems, Psychiatrics Expert Systems etc.
3. THE PROCESSES
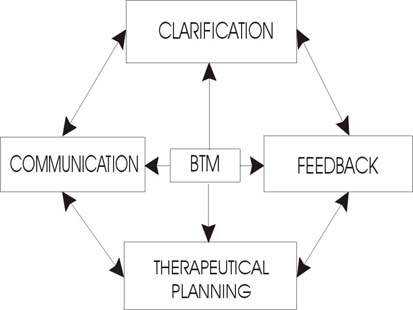
The BTM of the therapy as it was defined previously must be based on the particular four processes, clarification, communication, thrapeutical planning and feedback.
 |
Clarification
At many times the medical rules, which assure useful guides, in practice are not easily translated. This problem also exists because the patient at most of the times does not know his real condition. So the psychiatrist, with a danger to be expiatory victim is called to give clarifications in order to perform a beneficial consent around the therapy.
This effort of him, makes him use many times three different languages. At the beginning, he uses the typical scientific language when he cooperates with his colleagues and the nursing stuff, with the known problems of terminology and bounds. The populized scientific language, when he responds to the familiar person of the patient, considering their psychic and their knowledge level. Finally he uses “special” language for his patient.
The psychiatrist, also, needs to examine what was told and what was not in order to gain consensus for the implication of the therapeutical program.
Communication
By announcing the therapeutical program to the patient (if this is possible) and to his familiar persons, the psychiatrist must communicate the personal purposes (goals) and estimate their results in the future. But the familiar persons of the patient are not always ready and trained to participate in this communication. Therefore the psychiatrist have to establish a communicative pattern.
As phrase space can be determined the pattern of the communication where the problems and their solutions for the family are impressed. The relations are preserved through the equilibrium between the members express fear of love, proximity of remoteness, desire of abhorrence.
Therapeutical planning
This process helps the psychiatrist to complete the plans of all the parts of the therapeutical program in order to avoid conflict situations and rivalries.
For the beginning, there are two collided attitudes in the psychiatrist, the one of the researcher and the other of the observer – doctor. According to the first the psychiatrist must exam what exactly happens, which is the real problem, what exists behind of what he sees, what is the error. According to the second the psychiatrist must be in wakefulness towards the different reactions of the patient. What illusions, what memories come up and what is their relation?
The psychotherapeutic process affects the bounds / limits between the patient and the psychiatrist. That’s why there must be a control of the environment which becomes from the therapeutical procedure.
Feedback
When the therapeutical process is not successful and the patient’s condition is not improved, with simultaneously relief of the other factors (for example family, environment), then the planning must be reexamined before all the efforts get lost in the whirlwind of the parameters.
So this process allows the psychiatrist, with the aim of the feedback, to proceed to reviews of the therapeutical program and to value the success level of its different parts.
Because of the feedback process the BSC is called Dynamic. The changes and the reviews of the Dynamic BSC make the therapeutical program works better.
4. CONCLUSIONS
The unexpected of the psychic crisis can not be faced easily if there is not any organized plan. The fact that the balanced plan uses at the simultaneously four points of view for the therapy, decreases the percentage of failure. Moreover if one of the four perspectives will not work correctly, then the whole effort can be overturned, which does not happens to the other branch of Medicine.
The Balanced Treatment Model Allows:
The model of system interaction presented here has several advantages over traditional models. First, it is capable of specifying the conditions in which structural changes due likely to occur (far from equilibrium). Second, it specifies the mechanisms through which changes take place (nucleation, bifyrcation), and third, it specifically connects disfunctional patterns of interaction.
References
1)Bütz M, Champerlain L, Mc Cown, 1997, in Strange attractors, WILEY, NY,
2) Efraim J, Lukens M, Lukens R, 1990, in Language structure and change, W.W. NORTON, USA,
3)Kenny V, 1987, Anticipating autopoiesis: personal constructing psychology and self organizing systems, www.oikos.org/vincautopo.html
4)Koopmans M, 1995, Application of chaos theory to family interaction, http://hermes-op.com/inscirev/,
5)Koopmans M, 1997, Schizophrenia and the family: double bind theory revisited, http://goerter.org/dynapsyc/1997/koopmans.html
6)Masterpasqua F, Perna P, 1997, The psychological meaning of chaos, APA, USA,
7)Koopmans M, 1998, Chaow Theory and the problem of change in family systems, Non Linear Dynamics, Psychology, and Life Sciences, 2 (2): 133-148,
8)Lemay P, Dauwalden J-P, Pomini V, Bersier M, 199 , Quality of life: a dynamic perspective, in Nonlinear dynamics in human behaviour, Sulis W, Combs A, edy, World Scientific, Singapore.
9)Terpstra M, 1997, Illness as relationship, http:/home.earthlink.net
| Discussion Board | Your Symposium |